
Introduction: We previously reported that acute ingestion of 600 mg/kg body mass of a ketone monoester (KE) supplement increased heart rate (HR) and ventilation during submaximal constant-load cycling compared to placebo (1). The mechanistic basis for the increased cardiorespiratory stress is unknown but could be related to blood acidosis (2,3) and in turn affect cardiac output (Q̇).
Aims/objectives: The present case study examined the effect of increasing blood ketone bodies and manipulating pH on Q̇ during exercise. It informed the design of a larger comprehensive project that is ongoing (n=15). We hypothesized that KE versus placebo ingestion would increase Q̇ during exercise and that supplementing the KE with a blood pH buffer would attenuate this response.
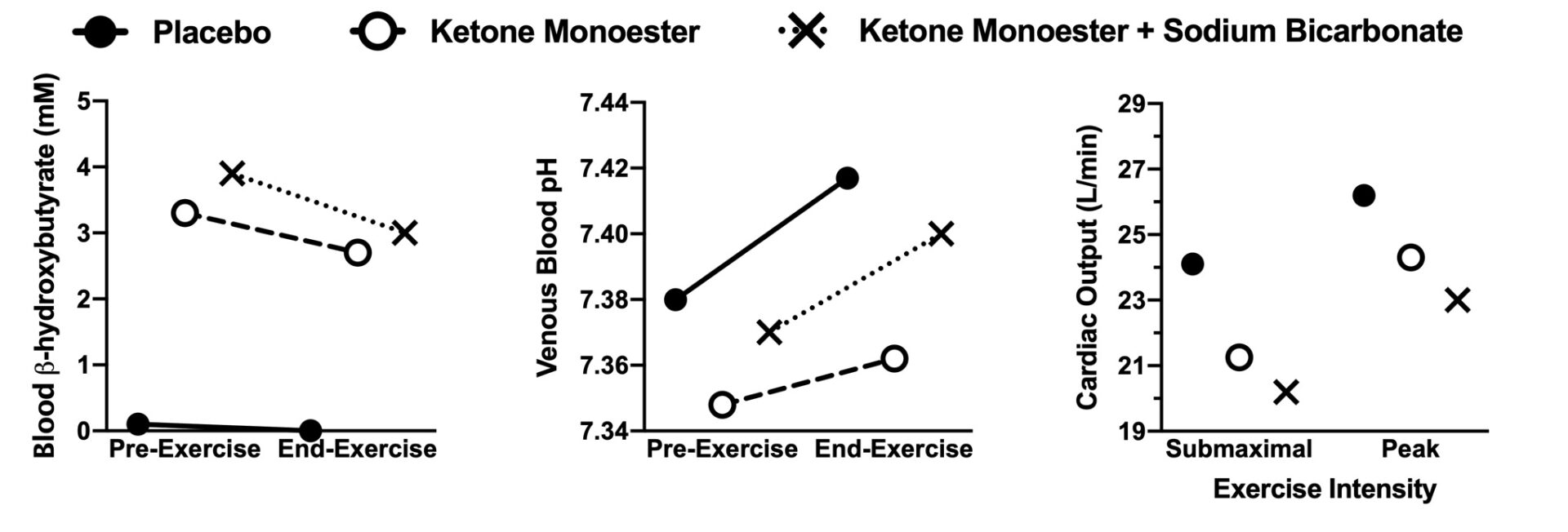
Methods: A male competitive triathlete (21 y, 74 kg) ingested either 0.6 g/kg of KE or a flavour-matched placebo, and 0.2 g/kg body mass of sodium bicarbonate (BICARB) or a salt control. The various manipulations created three experimental conditions: low ketone bodies and neutral pH (placebo), high ketone bodies and acidic pH (KE), and high ketone bodies and neutral pH (KE+BICARB). This was verified through venous blood gas analysis (EPOC, Siemens, Canada) (Figure 1). After supplementation, the participant cycled on an ergometer (Excalibur Sport v2.0, Lode, the Netherlands) for 30 minutes at ventilatory threshold intensity. HR was recorded throughout (Polar Electro model A300, Finland), expired gases were collected from 10-20 minutes using a metabolic cart (Quark CPET, COSMED, USA), and Q̇ was measured in duplicate at ~25 and ~29 minutes using inert gas rebreathing (Innocor, Innovision, Denmark). The constant-load exercise period was followed by an incremental protocol to fatigue for determination of peak oxygen uptake (VO2peak) and peak Q̇ peak as we have described (4). All procedures were approved by the Hamilton Integrated Research Ethics Board (#12811).
Results: During constant-load exercise in both KE-supplemented trials HR was ~8% higher (KE=158, KE+BICARB=156) compared to placebo (145 beats/min) and ventilation was 10% higher (placebo=102, KE=114, KE+BICARB=111 L/min). In contrast, Q̇ was ~15% lower in KE (20.9) and KE+BICARB (20.2) compared to in placebo (24.1 L/min) (Figure 1). This change in Q̇ exceeded day-to-day variability determined using Q̇ measured in duplicate on two separate days without nutritional manipulation (day 1=22.7, day 2=22.0 L/min, coefficient of variation=2.4%). VO2 varied by <1% between conditions (placebo=4.16, KE=4.15, KE+BICARB=4.19 L/min). Estimated arterial-venous oxygen difference during constant-load exercise, calculated using the Fick principle, was higher in both KE supplemented trials compared to placebo (placebo=172, KE=195, KE+BICARB=208 ml/L). Peak Q̇ was also 8-12% lower in the KE supplemented trials (KE=24.3, KE+BICARB=23.0) compared to placebo (26.2 L/min) (Figure 1). VO2peak (placebo=5.73, KE=5.57, KE+BICARB=5.45 L/min) and peak power output (placebo=470, KE=458, KE+BICARB=451 Watts) were also lower in the KE supplemented trials compared to placebo. Peak HRs were placebo=177, KE=181, and KE+BICARB=177 beats/min.
Conclusions: This case study suggests that KE supplementation, independent of blood acidosis, reduced Q̇ during both submaximal and peak exercise. VO2 was maintained during submaximal exercise potentially related to increased HR and oxygen extraction whereas VO2peak and peak power output were seemingly reduced.
Biomedical Basis of Elite Performance 2022 (University of Nottingham, UK) (2022) Proc Physiol Soc 49, PC32
Poster Communications: Acute exogenous ketone body supplementation reduces exercise cardiac output independent of blood acidosis: A case study
Devin McCarthy1, William Bostad1, Douglas Richards2, Martin Gibala1
1 Department of Kinesiology, McMaster University 2 Department of Medicine, McMaster University
View other abstracts by:
Where applicable, experiments conform with Society ethical requirements.