
Topographic cortical maps are essential for spatial localisation of sensory stimulation and generation of appropriate task-related motor responses. Somatosensation and nociception are finely mapped and aligned in the adult somatosensory (S1) cortex1. In neonates, a whole-body map of innocuous mechanical stimulation develops in S1 over the early postnatal period2, and although cortical responses to a noxious mechanical stimulus have been recorded from 28 weeks using functional near-infrared spectroscopy (fNIRS)3, the topographic representation of this activity has not yet been mapped. We propose that in infancy, when pain behaviour is disorganised and poorly directed4, nociceptive maps are less refined compared to somatosensory maps.
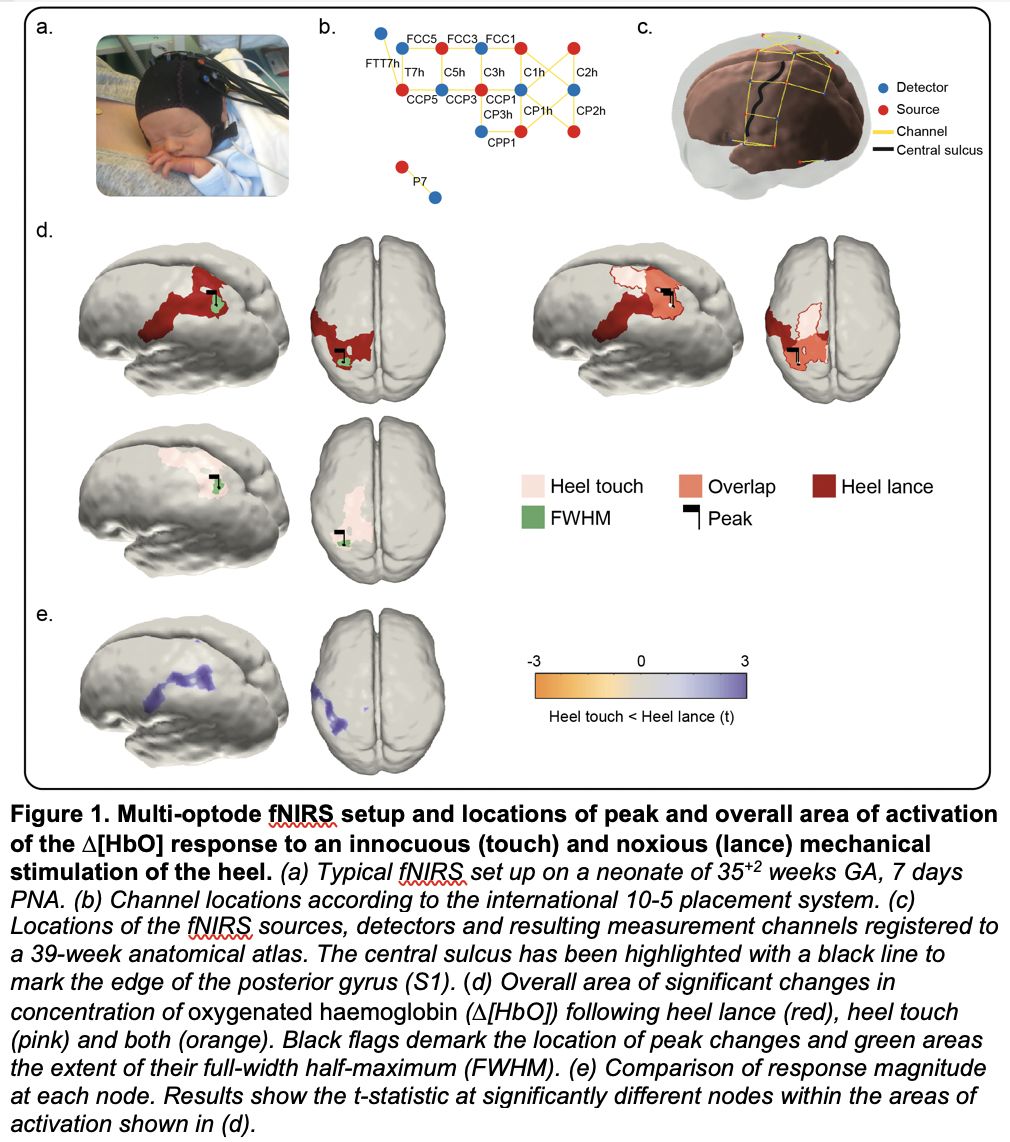
We used multi-optode fNIRS to map the haemodynamic response across the sensorimotor cortex following noxious (clinically-required heel lance) and innocuous (touch of the heel and hand) mechanical stimulation in 32 newborn infants (35-42 gestational weeks at birth, 0-7 days old, 12 female). Using channel-space and source reconstruction, we assessed the latency, location, magnitude, and topographic pattern of cortical activation following each stimulus. Ethical approval was given by the NHS Health Research Authority (London – Surrey Borders) and the study conformed to the standards set by the Declaration of Helsinki.
There was a significant localised increase in average concentration of oxygenated haemoglobin (D[HbO]) following touch of the heel (maximum change of 0.35 μM at 15.8 s post-stimulus) and hand (0.33 μM at 9.2 s), from baseline (-500 – 0 s pre-stimulus; Bonferroni-correct t-tests; p<.01), at locations consistent with the S1 regions representing the foot and hand respectively. Conversely, there was a widespread D[HbO] increase following the heel lance, which topographically overlapped with both the heel and hand touch responses. Non-parametric permutation analysis in source-space revealed that heel lance and touch elicited a peak increase at the same latency and location (Euclidean distance between peaks = 1.65mm, p=.156; difference in peak latency = 2s, p=.358), however the response was significantly larger (maximum D[HbO]: 16.06 vs 5.43 μM, p=.001) and the overall area of activation more widespread following lance (D[HbO] overall area: 455.27 vs 259.51 mm², p=.009). Importantly, the two responses only partially overlapped (in S1 region representing the foot), and while the heel touch response extended towards the motor cortex, the heel lance response extended towards more ventral regions of S1.
The widespread S1 nociceptive topography discovered here implies that nociceptive processing in the infant S1 is not somatotopically organised, consistent with their poorly directed pain behaviour. Heel lance is one of many skin-breaking procedures commonly performed in neonatal hospital care and this study reveals the extent of cortical activation that follows just one of such noxious procedure. This contrasts with innocuous mechanical stimulation, such as touch, which activates a spatially restricted and somatotopically defined cortical area.
Sensory Signals (The Royal College of Physicians, London, UK) (2022) Proc Physiol Soc 50, C06
Oral Communications: Widespread nociceptive maps in the human neonatal somatosensory cortex
Laura Jones1, Madeleine Verriotis1, Robert Cooper1, Maria Pureza Laudiano-Dray1, Mohammed Rupawala1, Judith Meek2, Lorenzo Fabrizi1, Maria Fitzgerald1
1University College London, London, United Kingdom 2University College London Hospitals, London, United Kingdom
View other abstracts by:
Where applicable, experiments conform with Society ethical requirements.