
Suited subjects submersed under cold-water experience ECG arrhythmias during and after volitional apnoea (1). We studied 32 healthy men immersed in cold (11°C) water, wearing trunks (mean(s.d.) age 21(3.5) years, height 1.78(0.09) m, mass 76.6(10.6) kg). Two hours before study, subjects rested, refrained from smoking, eating and drinking caffeinated drinks. Seated subjects completed two breath-holds in air (23.5(0.23)°C) wearing nose clip and mouthpiece; inspiratory frequency (fR) and volume (VI ; turbine), endtidal PCO2 was recorded. Three-lead electrocardiogram recorded lead II. Breath-hold duration (BHair:time between onset of last breath prior to breath holding, and onset of expiration) averaged 45.8(15)s. Arrhythmias were not seen during or following BHair. Subjects were winched above water for 2 min; they then again breath-held, and over 28s were lowered into water at 8m min-1 to clavicular level (total immersion duration 2.5 min). BHwater averaged 22.7(12.3)s, significantly less than BHair (p<0.001; paired t test, df=31). During BHwater, minor bradycardia was seen. Following BHwater, hyperventilation (fR 41.7(18.3)breaths/min, nadir PCO2 20.04(6.3)mmHg) and tachycardia occurred in all subjects (HR 115(3)1/ min); supraventricular and ventricular arrhythmias occurred in 20/32(63%) and 4/32(13%) subjects respectively, lasting a few seconds and usually in the first 10s after breathing recommenced. Two subjects had both supraventricular and ventricular arrhythmias transiently. Sinus tachycardia lasting about 30s was seen in 8/32 subjects, uninterpretable traces contaminated by shivering EMG and movement artefact occurred in 2 subjects. Arrhythmias were noted on occasion to be linked to respiration. A second group of 4 men (19-27 years), each studied thrice, breathed freely during cold immersion. Both groups showed tachycardia during cold immersion. However, only 1 free breathing subject on only 1 trial showed arrhythmias(coupled supraventricular ectopic beats). Since both groups are subject to the same hydrostatic and cutaneous cold stimulation during immersion, neither of these mechanisms per se are the origin of increased arrythmias seen following breath holding. They may be due to release of breath hold and consequent vagal stimulation, in a cold milieu. Under natural conditions, the nature and timing of cold immersion arrhythmias depend on which of 3 factors pertain: 1. Facial stimulation, producing bradycardia; 2. Cold, producing tachycardia; 3. Breath holding, producing supraventricular arrhythmias on release in cold water. Significant hypocapnia and ECG arrhythmias occur following breath holding during cold-water immersion, in healthy subjects wearing normal swimming attire.
University of Bristol (2005) J Physiol 567P, PC98
Poster Communications: ECG arrhythmias after voluntary apnoea during head-out cold water immersion
Datta, Avijit K; Barwood, Martin; Tipton, Michael J;
1. Institute of Biomedical and Biomolecular Sciences, University of Portsmouth, Portsmouth, United Kingdom. 2. Respiratory Centre, Portsmouth Hospitals NHS Trust, Portsmouth, United Kingdom.
View other abstracts by:
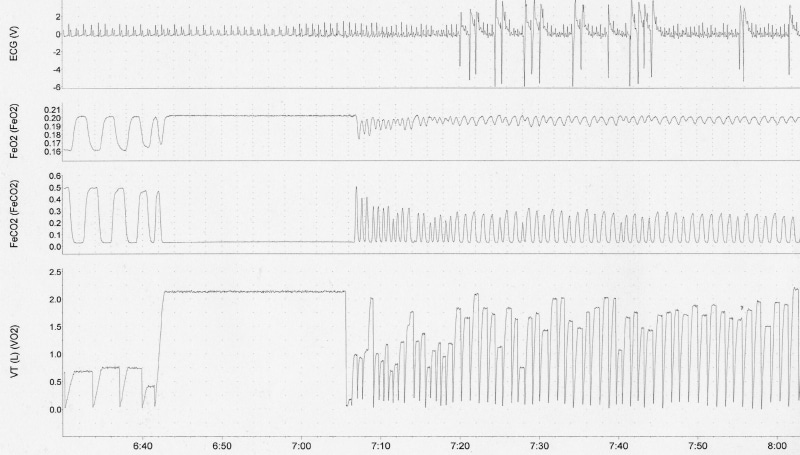
Figure 1. ECG of single subject showing sinus tachycardia and ventricular arrhythmias following break of breath hold during cold immersion. Breath hold time is diminished by cold shock to only 22 s with subsequent hyperventilation and hypocapnia.
Where applicable, experiments conform with Society ethical requirements.