
The phenomenon of myocardial ischaemic preconditioning (IPC) whereby brief periods of non-lethal ischaemia offer protection against any subsequent ischaemia/reperfusion injury was first described by Murry et al. (1986). Despite numerous descriptions in the literature of triggers for IPC, the exact mechanism by which it protects the heart remains unclear. Many of the endogenously released agents have been linked to downstream cellular signalling pathways involving Protein Kinase C (PKC). The activation of PKC with Phorbol 12-myristate 13-acetate (PMA) mimics IPC in whole heart as well as in isolated cells. Conversely, inhibitors of PKC prevent IPC. In this study we have used PMA to impart cardioprotection to rat isolated ventricular myocytes or used an interrupted perfusion protocol on a heart canulated on Langendorf equipment to mimic ischaemia in the whole heart. Immunohistochemical experiments on isolated cardiac cells showed that pre-treatment with PMA (10 μM for 10 minutes) caused translocation of all PKC isoforms from the cytosolic to particular fraction. Following interrupted perfusion IPC, PKC- α, γ, δ, ε, and λ/ς translocated to the particulate fraction suggesting the involvement of these isoforms in the protective process. Using cell permeant Tat-linked PKC isoform-specific inhibitor peptides, we investigated the effect of specific PKC isoforms on the time to contractile failure, rigor contracture and the recovery of contractile function after a metabolic inhibition/reperfusion (MI) protocol on isolated cardiac myocytes. Briefly, cells were perfused with normal 2mM Ca2+ Tyrode solution (2CaT) for 5 minutes, 7 minutes with substrate-free 2CaT with 2 mM cyanide and 1 mM iodoacetate, thereperfused with 2CaT. Myocytes were pre-treated with 100 nM inhibitor peptide for 15 minutes and 10 μM PMA for the last 10 minutes. Cells were then subjected to electric field stimulation at 1 Hz to measure contractile failure, rigor and contractile recovery, or measured using patch clamp electrophysiology to measure time to action potential failure. These data, and recordings from patch clamp electrophysiology (not shown), demonstrated that there is a marked cardioprotection imparted by PMA or by IPC of whole hearts. Both protocols delay the time to contractile failure, delay the time to rigor contracture and also improve the survival on reperfusion. Inhibition of PKCγ and ε both markedly reduce the PMA induced preconditioning suggesting that they both impart cardioprotection.
University of Manchester (2010) Proc Physiol Soc 19, PC105
Poster Communications: Multiple protein kinase C isoforms contribute to cardioprotection
R. D. Rainbow1, R. I. Norman1, D. Hudman2
1. Cardiovascular Sciences, University Of Leicester, Leicester, United Kingdom. 2. Medical and Social Care Education, University Of Leicester, Leicester, United Kingdom.
View other abstracts by:
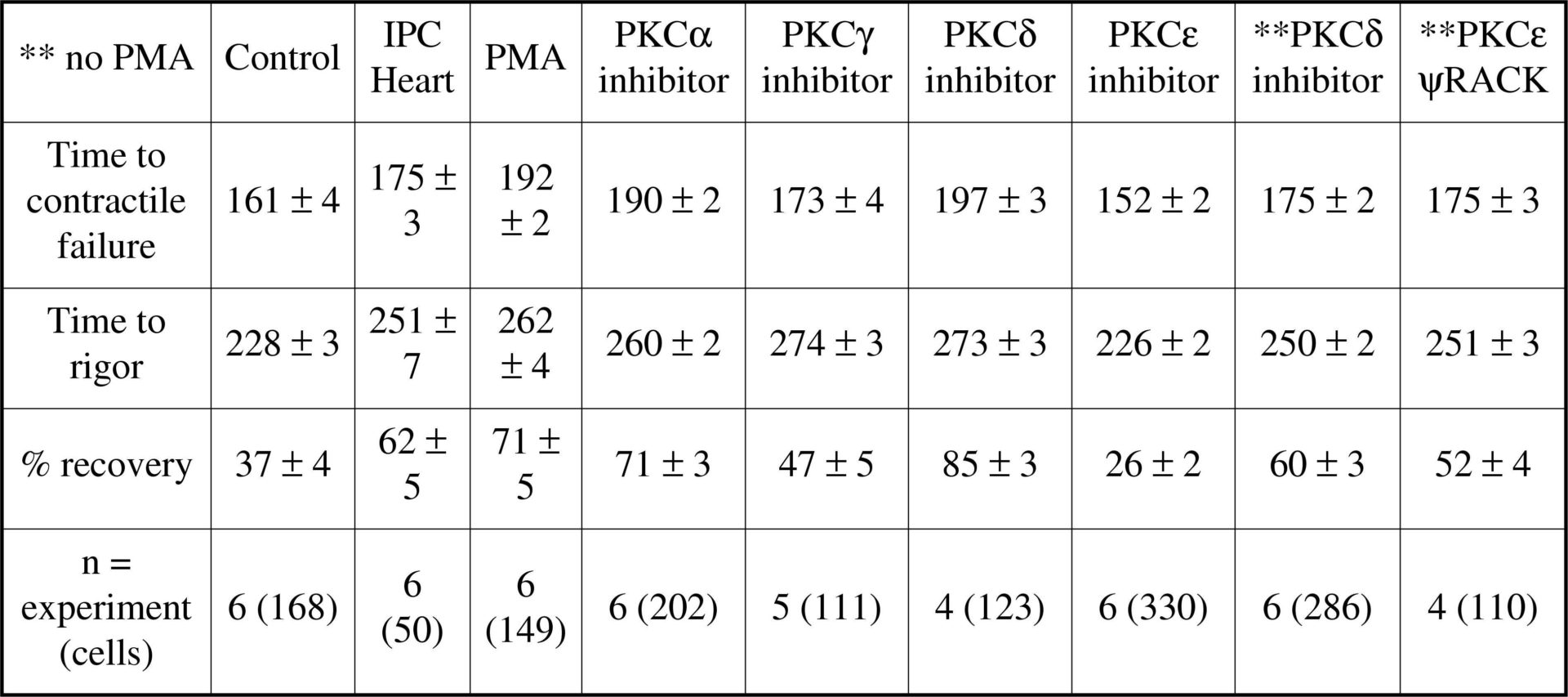
Contractile function studies on PMA pre-treated or IPC whole hearts with PKC-isoform specific inhibitor peptides<#13>
Where applicable, experiments conform with Society ethical requirements.