
Physiology News Magazine

Why do we have two noses?
Features
Why do we have two noses?
Features
Ron Eccles
Common Cold Centre, Cardiff University, UK
https://doi.org/10.36866/pn.102.23
We have two eyes, two ears, two lungs and two kidneys but we always refer to THE NOSE in the singular and this singular terminology hides a wealth of unusual nasal physiology.

Try this simple experiment Place the ball of your thumb over one nostril and breathe in gently. Repeat the procedure with the other nostril. Notice anything? The first and obvious discovery is that you have two nasal passages and I would like to wager a bet that around 80% of you will find that you have asymmetrical nasal airflow with one side of the nose having a lower resistance to airflow than the other. Repeat this experiment in a couple of hours and many of you will make an even more unusual discovery, and that is that the dominant airflow has changed from one side of the nose to the other.
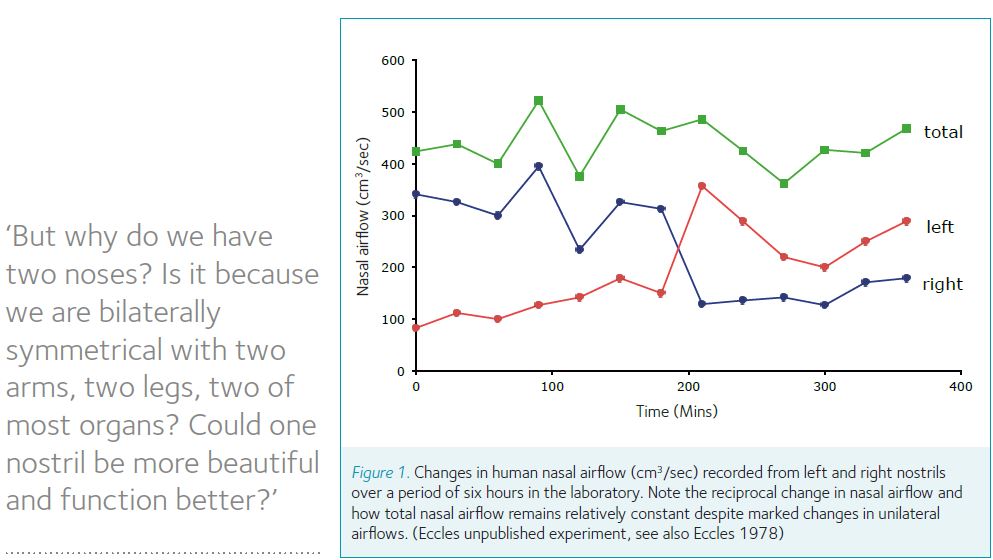
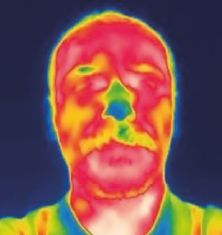
Experiments that record the nasal airflow from each nasal passage over a period of hours have described regular reciprocal changes in nasal airflow in man and this is often called a ‘nasal cycle’ like the one shown in Fig 1. If you take an infra-red photo of a moustachioed face on a cold day, it is possible to see that only one side is cooled by the nasal airflow (Fig 2).
Watch a cow or horse or sheep on a cold winter day and you can often see the same asymmetry of nasal airflow in the expired steamy nasal airflow. Studies on rats, cats, dogs, and pigs have clearly shown that nasal airflow is normally asymmetrical and that there is a reciprocal relationship of nasal airflow, which alternates over a period of hours. Elegant physiological and anatomical studies in the rat and rabbit clearly showed the asymmetrical nasal airflow, by looking at condensed nasal airflow patterns on a cold metal mirror in tranquilized rats and rabbits and then following up these experiments with post mortem examination of the nasal swell bodies (venous sinuses and cavernous spaces in the mucosa of the conchae and the septum) (Bojsen-Moller & Fahrenkrug, 1971).
When suffering from a common cold you may remember one side of your nose becoming so blocked that you could not breathe through it and the other remaining open so that you only breathed through one side of the nose. You probably did not feel up to doing much experimentation when suffering from this common cold but if you had been observant you would have noticed the dominant airflow to change sides with a periodicity of a couple of hours. In a study on subjects with common cold we demonstrated that during a cold one side of the nose becomes very blocked whilst the other side remains open (Eccles et al., 1996). The unilateral blockage was explained by an increased filling of nasal veins due to inflammation, with this increase in blood flow superimposed on an asymmetrical sympathetic vasoconstrictor tone to the nasal veins.
Ever had one side of the nose block up when lying in bed? Lie on the left side and the left nasal passage blocks up, turn over and lie on the right side and the right nasal passage blocks up. Asymmetrical skin pressure triggers reflex changes in nasal airflow so our upper nasal passage always has the dominant airflow whilst the nasal passage at risk of occlusion from the ground or pillow blocks up. Human studies have demonstrated that lying down on one side stimulates slowly adapting pressure receptors on one side of the body to trigger a nasal reflex that opens one side of the nose and closes the other (Haight & Cole, 1986).
Applying a crutch to one armpit causes nasal airflow on that side to decrease and airflow on the other side to increase. This reflex was studied in healthy volunteers and showed that application of the crutch caused reciprocal changes in nasal airflow (Davies & Eccles, 1985). Our experiments have shown similar reciprocal effects on nasal airflow in a study on healthy volunteers by asking them to squeeze a plastic ball in the axilla (Preece & Eccles, 1993). In the dim and distant past Indian mystics used a small crutch (yoga danda) to alternate nasal airflow from one nasal passage to the other, and modern day yoga students of pranayama uses a yoga danda to control nasal airflow and alternate the dominance of nasal airflow from one side to the other at will.
Cats provide some answers. Our studies on the anaesthetised cat have shown that nasal airflow is controlled from the hypothalamus via the sympathetic nerves that cause constriction of large veins lining the nose. Electrical stimulation of alternate sides of the brainstem region in the cat demonstrated that there are control half centres in this brain region that regulate the sympathetic nerves to the nose and act as a flip-flop mechanism to control nasal airflow (Bamford & Eccles, 1982).
But why do we have two noses? Is it because we are bilaterally symmetrical with two arms, two legs, two of most organs? Could one nostril be more beautiful and function better? Surely a single large nostril placed in the centre of the face could function as effectively as is the case for the mouth where one opening serves us very well. It could take us a little while to appreciate the beauty of a single nostril as opposed to the beauty of our paired and smaller nostrils but I feel this would grow on us, especially us physiologists, as a single large nostril would have better aerodynamics and offer less resistance to airflow than our two smaller nostrils. The nose does present a considerable resistance to airflow- around two thirds of the resistance to airflow of the whole airway from nostril to alveoli. Most of the work of breathing is related to moving air through the nose and this is the price we pay for filtering and conditioning the air we breathe.
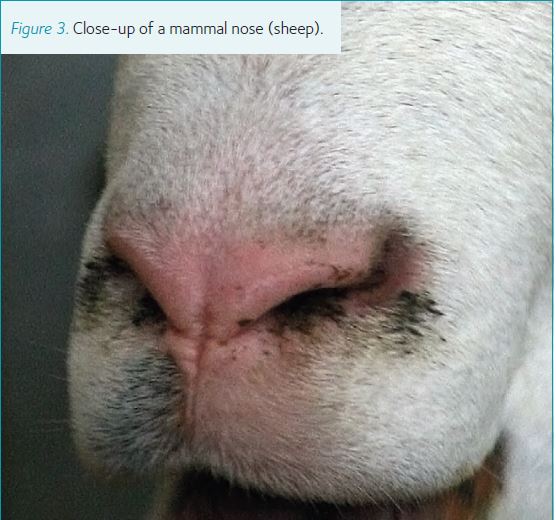
There’s a twist to the nose, and the human nose is unique in two ways. Visit the zoo and get close up to the bars to get a very close look at the nose of any mammal (such as a sheep as illustrated in Fig 3). The nostrils come straight out of the face and the airflow is twisted as it passes through the nostril in a cork screw fashion. This twist aids filtration of particulate matter as dust is spun out of the airstream and deposited in the nose.
This is quite different from the human nose, which is unique in that the nostrils point downwards, unlike any other mammal, including our close relatives the chimpanzee and gorilla. Maybe the downward direction of the nostrils is an adaptation to our upright posture? However, we still have a bend rather than a twist to the nose to aid filtration as the airflow passes up through the nostril and then turns at a right angle to enter the nasal passages at the narrowest point of the nose and whole airway, the nasal valve. The change in direction of nasal airflow, and the decrease in velocity after the nasal valve, spin out any dust and acts as a very efficient filtration mechanism. Another unique feature of the human nose is the presence of small hairs or vibrissae, with more in men than women, as the development is sex hormone dependent. No other mammal has these vibrissae and they appear to have no function apart from acting as a barrier to flies and small insects that may creep into the nose and trigger sneezing.
But why do we have two noses? For an air conditioning unit that works 24/7, 365 days a year it makes sense to have two units in parallel and alternate the airflow from one side to the other over a period of hours. Two noses are therefore very useful as one can go through a rest and cleansing cycle whilst the other takes over the dirty and damaging work filtering and conditioning the 10-20,000 litres of air we breathe in every day.
Having two noses means that when we have a common cold caused by viral infection one side of the nose can become inflamed and blocked whilst the other manages all our airflow.
Inflammation is the natural response to infection as more blood flow is diverted to the infected area, but there is also another benefit of closing one nasal passage related to nasal temperature. The normal temperature of the nasal epithelium is around 33C and common cold viruses have adapted to this temperature and replicate best at around 32C. This is why all early attempts to culture common cold viruses failed as they were incubated at 37C. The inflammation that blocks one nasal passage raises the nasal temperature to 37C and this may help us to throw out the viruses as they do not replicate well at this higher temperature (Papadopoulos et al., 1999).
Another benefit of having alternating congestion and decongestion of the large veins in the nose is that when the large veins on the blocked side of the nose contract, they squeeze out a plasma exudate containing antibodies that washes and cleans the nose and also helps to neutralise viruses and this is another benefit of the so called ‘nasal cycle’ (Eccles, 1996).
So, two noses are better than one! Having two noses may have some functional significance. Two noses allow for periods of asymmetrical airflow and therefore allow cycles of rest for the hard working air conditioners. Two noses also allow for periodic obstruction of one nasal passage without compromising ventilation and this may help in overcoming viral infection by raising the nasal temperature.
References
Bamford OS, Eccles R (1982). The central reciprocal control of nasal vasomotor oscillations.
Pflugers Archiv. 394, 139-143.
Bojsen-Moller F, Fahrenkrug J (1971). Nasal swell bodies and cyclic changes in the air passages of the rat and rabbit nose. J Anat 110, 25-37
Davies AM, Eccles R (1985). Reciprocal changes in nasal resistance to airflow caused by pressure applied to the axilla. Acta Oto-Laryngol 99, 154-159
Eccles R (1996). A Role For the Nasal Cycle In Respiratory Defense.
European Respiratory Journal 9 (2), 371-376
Eccles R, Reilly M, Eccles KSJ (1996). Changes in the amplitude of the nasal cycle associated with symptoms of acute upper respiratory tract infection.
Acta Otolaryngol 116 (1), 77-81
Haight JS, Cole P (1986). Unilateral nasal resistance
and asymmetrical body pressure.
J Otolaryngol Suppl 6, 1-31
Papadopoulos NG, Sanderson G, Hunter J, Johnston SL (1999). Rhinoviruses replicate effectively at lower airway temperatures. J Med Virol 58 (1), 100-104
Preece M, Eccles R (1993). The effect of pressure and warmth applied to the axilla on unilateral nasal airway resistance and facial skin temperature.
Acta Oto-Laryngol 113, 777-781