
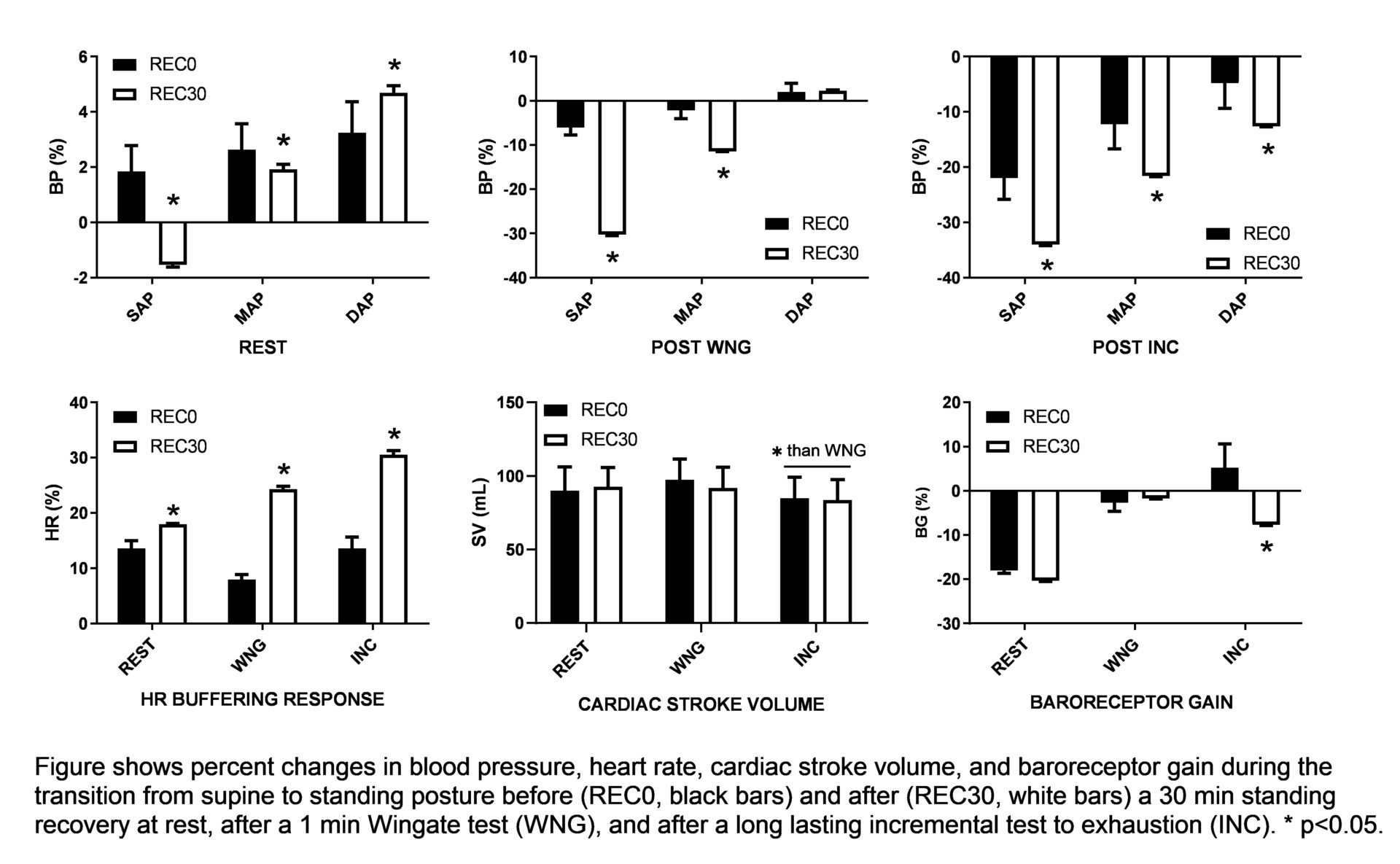
Effective control of vascular conductance after exercise is essential to avoid post-exercise hypotension (1). Such a vascular control is due to a balance between sympathetic vasoconstriction and metabolic vasodilation (2). Previous evidence suggests that immediately after exercise there may be relatively greater SNS effects on vascular control (3) associated with persisting vasodilation and reduced vasodilator function (4). As the recovery progresses, sympathetic vasoconstriction effects become less evident and vasodilator function normalizes. Indeed, although most documented hypotension episodes occur within 10 minutes after exercise, athletes often report presyncope symptoms over 30 minutes of recovery (5). Thus, this project assessed the cardiovascular adjustments to posture changes immediately after exercise than after a 30 min recovery. In compliance with the ethical standards, 15 male subjects practicing different sports (weightlifting, tennis, soccer, cycling, running) were passively tilted twice (1 min supine and 1 min upright) before and after a 30 min standing still recovery (REC30; if not interrupted by pre-syncopal symptoms). This was performed at REST as well as after a 1-min Wingate test (WNG) and after a long-lasting incremental test to voluntary exhaustion (INC; 15W / min). Such exercises were chosen to obtain two different levels of metabolic vasodilation in the immediate post-exercise period. During all phases of the experiments, beat-by-beat blood pressure (BP) and heart rate (HR) were collected continuously. Cardiac stroke volume (SV) was calculated upright just before both tilt tests through cardio-impedance analysis. Baroreceptor gain (BG) was calculated as ΔRR / ΔSAP. Percentage changes in systolic (SAP), mean (MAP), and diastolic (DAP) BP as well as in HR, and BG from supine to standing position were analyzed via 2-way repeated measures ANOVA. DAP and SV were considered related to peripheral resistance. Among all subjects, syncope (1) or presyncope (3) appeared only in weightlifters. In the other 11 subjects, REC30 consistently increased the heart rate buffering response to standing inclination (+5Δ%, +16Δ%, +15Δ%; all p<0.05; REST, WNG, INC) and augmented the SAP drop to the upright tilting (+5Δ%, +16Δ%, +15Δ%; all p<0.05; REST, WNG, INC). Pre-exercise MAP rose to standing transition more before (+2.5±0.8%) than after REC30 (-2±0.2%; p<0.05). Post-exercise MAP to standing transition fell immediately after exercise (-2±2.1%, -12±4.3%; WNG, INC), but such a fall was much greater after REC30 (-12±1.1%, -22±1.4%; all p<0.05; WNG, INC). DAP increased to standing inclination at REST and after WNG, but dropped after INC (-5±4.9%) to a greater extent after REC30 (-14±1.1%; p<0.05). Post-recovery BG was lower (p<0.05) after INC only. SV was consistently lower (p<0.05) after INC than REST and WNG throughout the entire recovery period. Our data show that the standing transition from supine induces augmented hypotension after a 30 min standing recovery than immediately after exercise, which cannot be effectively counteracted despite an effective HR buffering response. Such an effect is greater after a long-lasting strenuous aerobic exercise compared to a short bout of supramaximal exercise and, according to DAP and SV data, enhanced hypotension may be due to ineffective control of the peripheral resistance.
Future Physiology 2021 (Virutal) (2021) Proc Physiol Soc 47, PC42
Poster Communications: Thirty minutes of standing recovery enhance post-exercise hypotension.
Alessandro Gentilin1, Enrico Tam1, Cantor Tarperi1, 2, Federico Schena1, Antonio Cevese1
1 University of Verona, Verona, Italy 2 University of Turin, Turin, Italy
View other abstracts by:
Where applicable, experiments conform with Society ethical requirements.