
Exhaustive high-intensity whole-body exercise (>90% VO2peak) elicits fatigue of the expiratory muscles that in turn impairs exercise tolerance (1, 2). A possible mechanism for this exercise limitation is a reflexively-mediated increase in sympathetic vasomotor outflow that compromises perfusion of limb locomotor muscles limiting their ability to perform work (i.e. ‘the respiratory muscle metaboreflex’). We investigated the effect of fatiguing expiratory muscle contractions on: 1) leg blood flow (QL); 2) leg vascular resistance (LVR); and 3) mean arterial pressure (MAP), heart rate (HR) and cardiac output (Q) in otherwise resting humans. On two separate days, twelve healthy adults (2 f; mean ± SD; age = 25 ± 4 y) performed expiratory resisted loaded breathing (ERL) at 2% (ERL-CONTROL) or 65% (ERL-FATIGUE) of maximal expiratory mouth pressure (MEP); ERL-CONTROL was performed for 5 min and ERL-FATIGUE was performed to task failure. On a third day, a subset of individuals (n = 5) performed ERL at 2% of maximal gastric pressure (PgaMAX) (ERLPga-CONTROL) for 5 min before undergoing ERL at 65% of PgaMAX (ERLPga-FATIGUE) to task failure; subjects were instructed to ‘breathe from their abdomen’ during each resisted expiration to specifically target the expiratory abdominal muscles. Breathing frequency was set at 15 breaths/min with a 0.5 expiratory duty cycle (TE/TTOT) for all ERL trials. MAP, HR and Q were measured continuously via finger photoplethysmography. QL was measured every 1 min by Doppler ultrasound and LVR calculated as MAP/QL. For all trials, expiratory muscle fatigue was assessed by measuring the pre- to post-ERL reduction in MEP. In addition, the reduction relative to baseline values in magnetically evoked gastric twitch pressure (Pgatw) was assessed in ERLPga-CONTROL and ERLPga-FATIGUE. There was no evidence of expiratory muscle fatigue in either control trial. QL, LVR, MAP, HR and Q were unchanged during ERL-CONTROL and ERLPga-CONTROL (P > 0.05). By contrast, MEP decreased by 19 ± 5% (P < 0.05) from before to after ERL-FATIGUE. Similarly, there was a 16 ± 6% and 14 ± 9% decrease in MEP and Pgatw, respectively, from pre- to post-ERLPga-FATIGUE. At task failure, MAP and HR were increased relative to resting values by 31 ± 10 mmHg and 28 ± 4 beats/min for ERL-FATIGUE and 18 ± 9 mmHg and 31 ± 10 beats/min for ERLPga-FATIGUE (all P < 0.05). Conversely, there was no significant change in Q during either fatiguing ERL trial. Group mean QL and LVR were unchanged from eupneic values during ERL-FATIGUE and ERLPga-FATIGUE (P < 0.05), despite considerable variability in individual responses to both tasks (Figure 1). In conclusion, these data do not support a reflexively-mediated reduction in QL and increase in LVR during fatiguing expiratory muscle contractions, despite large increases in MAP and HR, even when the expiratory abdominal muscles are specifically targeted.
Physiology 2019 (Aberdeen, UK) (2019) Proc Physiol Soc 43, PC132
Poster Communications: Cardiovascular consequences of fatiguing expiratory muscle work
T. A. Hardy1, M. P. Ribeiro2, G. K. Lyall1, K. M. Birch1, C. Ferguson1, B. J. Taylor1
1. School of Biomedical Sciences, University of Leeds, Leeds, United Kingdom. 2. Division of Translational Medicine, Federal University of Sao Paulo, Sao Paulo, Brazil.
View other abstracts by:
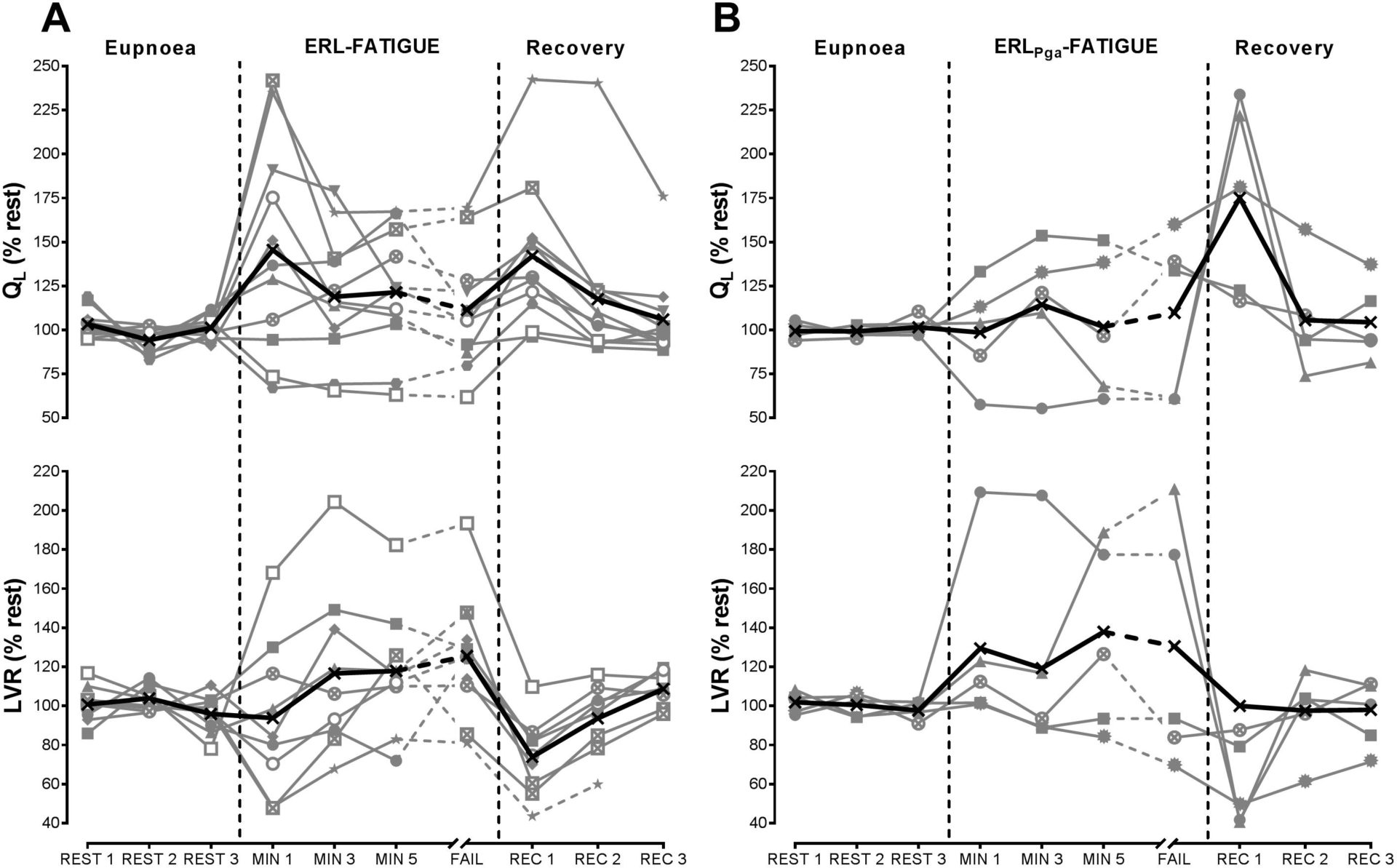
Figure 1. Leg blood flow (QL; top panel) and leg vascular resistance (LVR; bottom panel) during (A) fatiguing expiratory resistive loading targeting 65% of maximal expiratory mouth pressure (ERL-FATIGUE, n = 12) and (B) fatiguing expiratory resistive loading targeting 65% of maximal gastric pressure (ERLPga-FATIGUE; n = 5). Black lines represent group means; grey lines represent individual data. Female data are presented in open symbols.
Where applicable, experiments conform with Society ethical requirements.