
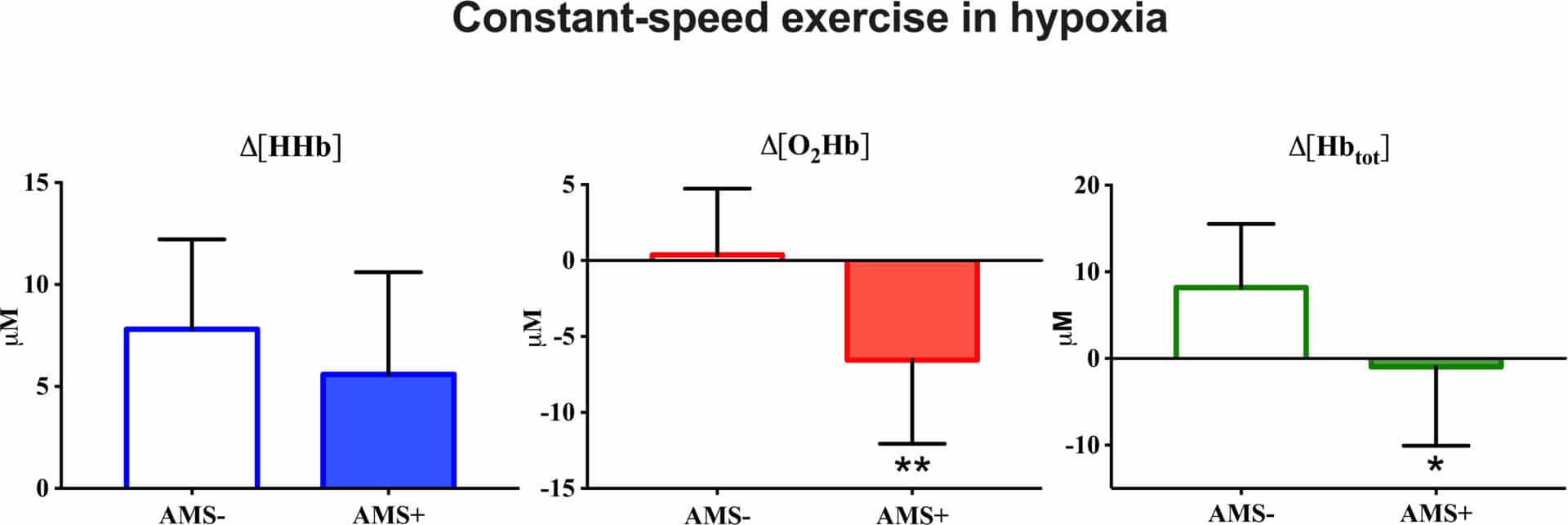
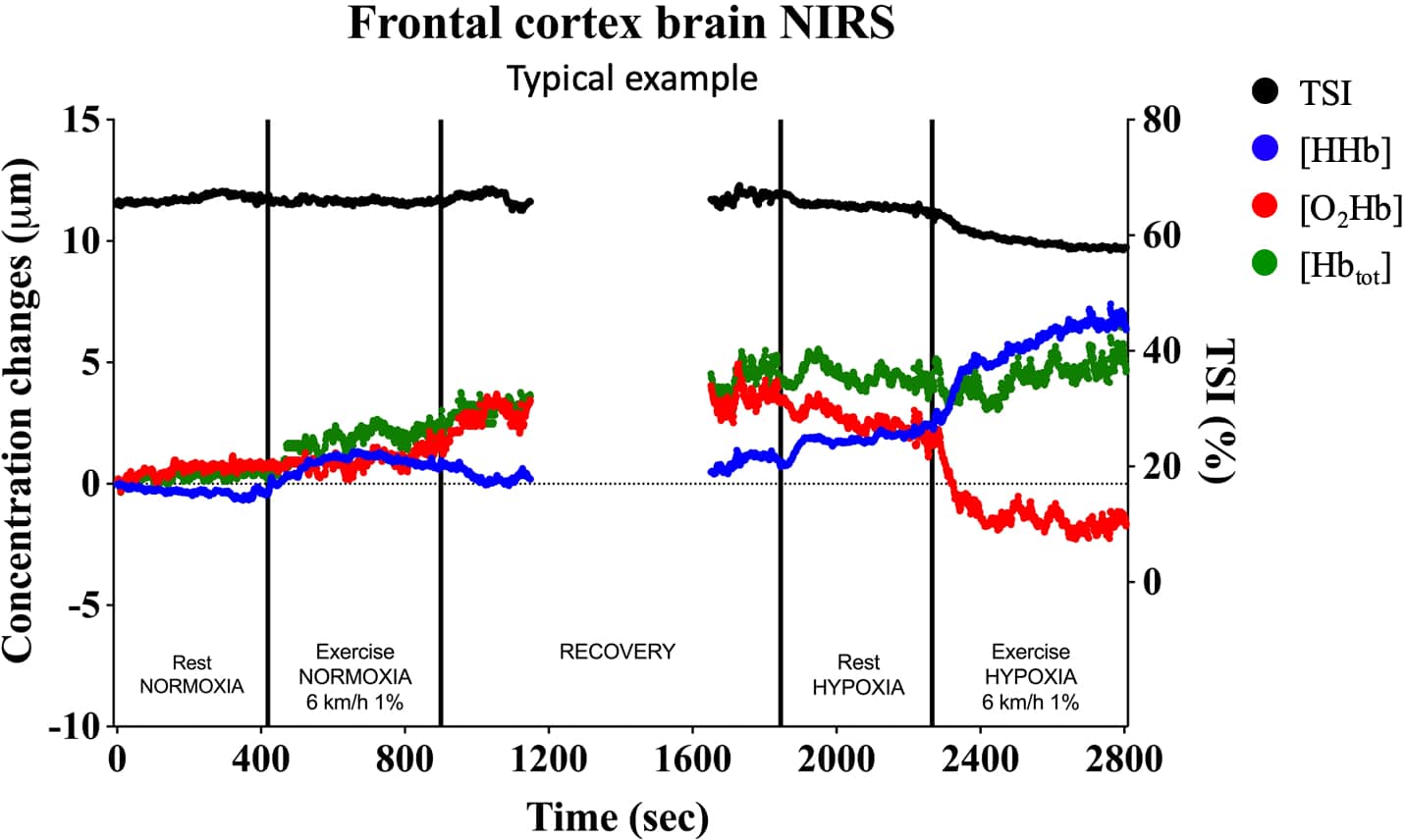
INTRODUCTION Acute mountain sickness (AMS) can occur in people who ascend above 2500m1. The underlying pathophysiology of AMS is not completely understood. Altered autoregulation of cerebral blood flow (CBF) and/or impaired brain oxygenation during hypoxic exposure may be involved in AMS occurrence2. Previous studies did not observe any difference in CBF between symptomatic (AMS+) or asymptomatic (AMS-) subjects at rest3. Since exercise affects CBF and oxygenation in normoxia, and hypoxia can exacerbate these modifications4, the aim of this study was to evaluate changes in cerebral oxygenation and microvascular blood volume during exercise in normobaric hypoxia and investigate possible association with AMS occurrence at high altitude. METHODS Twenty-two (15 men; 7 women) healthy young subjects (26±4yrs) were recruited for the study. Each participant completed the following exercise tests on a motorized treadmill: i) an incremental exercise to exhaustion (INCR); ii) two 8-minutes constant-speed exercises (CSE) at moderate intensity (below gas exchange threshold), one in normoxia (NORM) and the other in normobaric hypoxia (FiO2=0.13; HYPO). Breath-by-breath V’O2, V’CO2, and V’E were measured by metabolic cart. HR was measured using chest band. SpO2 was measured by finger pulse oximeter. Cerebral frontal oxygenation (HbO2), deoxygenation (HHb), and microvascular blood volume (Hbtot) were obtained by near-infrared spectroscopy (Fig.1). Occurrence of AMS, defined as a Lake Louise Scale score equal or higher than 3, was evaluated in the 24 hours following the arrival at Gnifetti hut (3647m), reached by cable car and two hours hiking. RESULTS During INCR, V’O2peak was 3.30±0.87L/min, corresponding to 48.8±8.5ml/kg/min. During CSE, subjects exercised at about 40% of V’O2peak. V’E and HR were significantly higher in HYPO (40.9±7.6L/min and 141±15bpm, respectively) vs. NORM (34.5±5.8L/min and 117±15bpm). SpO2 significantly decreased during HYPO (75±5%). As for cerebral NIRS-derived parameters, HHb, HbO2, and Hbtot did not change from resting values in NORM, resulting similar between AMS+ (n=8) and AMS- (n=14) subjects. In HYPO, HHb significantly increased (by about 3µM) from resting values in both AMS+ and AMS- subjects (Fig.2). Hbtot did not change from resting values in AMS+ subjects whereas it significantly increased (from 5.49±3.99 to 8.17±7.34µM) in AMS- subjects. HbO2 (0.37±4.36µM) significantly decreased from resting values (1.44±2.14µM) only in AMS+ subjects. CONCLUSION Subjects presenting symptoms of AMS at altitude seem to be unable to both increase microvascular blood volume and maintain oxygenation at cerebral level during exercise in acute normobaric hypoxia, suggesting these changes may underpin later development of AMS. Future studies should confirm these findings and investigate the underlying mechanisms.
Extreme Environmental Physiology (University of Portsmouth, UK) (2019) Proc Physiol Soc 44, C19
Oral Communications: Changes in cerebral oxygenation and microvascular blood volume during exercise in hypoxia and possible association with acute mountain sickness
G. Manferdelli1,2, M. Marzorati1, C. Easton2, S. Porcelli1
1. National Research Council, Milan, United Kingdom. 2. University of the West of Scotland, Hamilton, United Kingdom.
View other abstracts by:
Where applicable, experiments conform with Society ethical requirements.