
Respiratory muscle work is not generally thought to make a significant contribution to blood lactate concentration ([lac–]B) during exercise. When minute ventilation (VE) in maximal exercise is reproduced voluntarily at rest there is either no change in [lac–]B (Babcock et al. 1995) or a modest 0.5 mmolnull;l-1 increase (Martin et al. 1984). However, at rest lactate production by respiratory muscles may not be reflected by an increased [lac–]B due to clearance by other tissues. At maximal lactate steady state (MLSS), however, there is no ‘spare capacity’ for lactate clearance, thus further lactate efflux from respiratory muscles should accumulate in the blood. We thus examined the effects of volitional hyperpnoea on [lac–]B during exercise at MLSS. With local ethics committee approval and written informed consent, 7 healthy males (aged 25.6 ± 1.8 yr) were studied. A lactate minimum test (Tegtbur et al. 1993) was used to estimate MLSS cycling power, which was then resolved using at least two separate 30 min constant-load tests. Thereafter, a 30 min control trial (CT) at MLSS was performed. On a further occasion (experimental trial, ET) CT was mimicked except that from 20-28 min maximal volitional hyperpnoea was performed. Isocapnia was maintained by adding CO2 to the inspirate to maintain a constant end-tidal CO2, which was monitored breath-by-breath. PCO2 of arterialised venous blood (PaCO2) was determined and corrected for rectal temperature changes. Data were analysed using factorial ANOVA and expressed as mean ± S.E.M. Statistical significance was set at P < 0.05. MLSS power was 207 ± 8 W. Changes in VE and [lac–]B for the first 20 min of exercise were not different between CT and ET (Fig. 1). From 20-28 min VE during CT and ET was 87.3 ± 2.4 and 168.3 ± 7.0 lnull;min-1, respectively (P < 0.01), the latter being comparable to that achieved in the maximal phase of the lactate minimum test (171.9 ± 6.8 lnull;min-1). From 20-30 min [lac–]B during ET increased significantly (P < 0.05) by 0.9 ± 0.2 mmolnull;l-1 (+24.9%). There was also a slight 2.2 ± 0.8 mmHg increase in PaCO2 from 20-30 min in ET, which may have attenuated the increase in [lac–]B. This study shows that the work of breathing during heavy exercise influences [lac–]B, probably because of significant lactate production and release from respiratory muscles. However, respiratory muscle metaboreflex activation may have also compromised blood flow to, and thus lactate uptake by, locomotor muscles.
King's College London (2005) J Physiol 565P, C37
Communications: Contribution of exercise hyperpnoea to the blood lactate concentration of heavy endurance exercise
Johnson, Michael ; Sharpe, Graham ;
1. Division of Sports Science, The Nottingham Trent University, Nottingham, United Kingdom.
View other abstracts by:
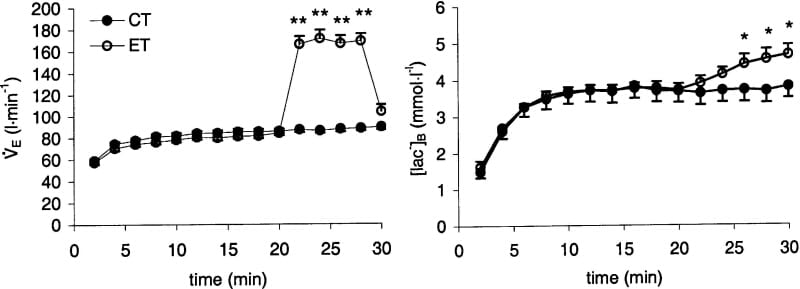
Figure 1. Changes in minute ventilation and blood lactate concentration during CT and ET. Significant difference between trials: *P < 0.05 **P < 0.01.
Where applicable, experiments conform with Society ethical requirements.