Muscle fatigue is referred to as a progressive reduction of force generated during muscle exertion due to any physical activity or exercise1. To compensate for the decline in force capacity of agonist muscles during sustained submaximal isometric contraction (sIMC), the net excitatory input to the motoneurons pool is increased to recruit additional motor units to maintain the force level until task failure. This common control of coactivation can lead to disproportionate rise in antagonist muscle activity2. Hand grip is commonly studied in non-fatigue tasks, and the most common synergistic pattern observed is coactivation of agonists and antagonists3. However, it remains unexplored if this activation pattern is affected.
In this study we used, the commonly used fatigue indicators root mean square (RMS), and median frequency (MDF)4, parameters of surface electromyographs (sEMG), to examine the process of failure during a sIMC task. Having established fatigue, we identified the pattern activity of hand and forearm muscles during the task.
Method: 5 healthy participants (aged 31.2 ± 6.41 years) performed a sIMC protocol to induce fatigue until failure of task, preceded by them generating maximal grip force (MGF) (3s) using their dominant hand. A Bluetooth-enabled handgrip dynamometer (SQUEGG, USA) was used to record the MGF, and to provide feedback to the subject when performing the sIMC task. The posture and position of the hand was maintained as recommended by the American Society of Hand Therapists5. Participants performed the sIMC maintaining a target force at 50% of MGF for 5 minutes with visual feedback. This was repeated twice with a 5-minute rest between each repetition. sEMG signals from 7 hand and forearm muscles was recorded. Each sIMC was split into two epochs of 30s each: early (the first 30s) and, final (the last 30s from the time of failure). All data is presented as mean ± standard error.
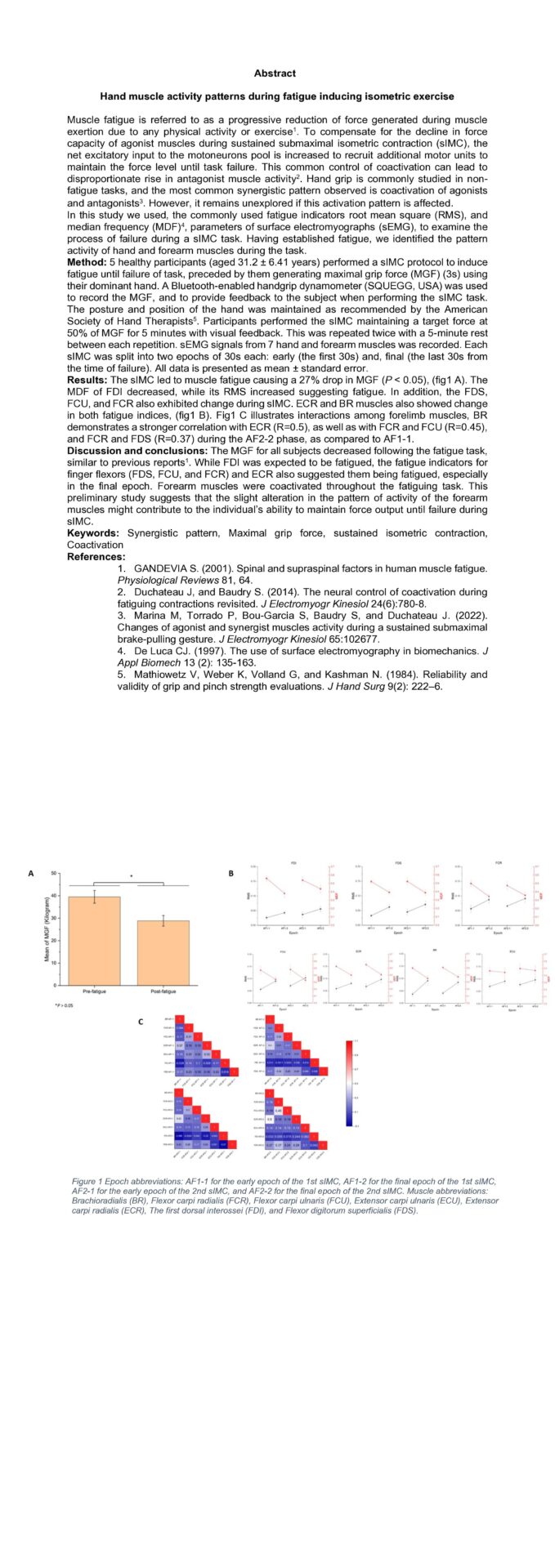
Results: The sIMC led to muscle fatigue causing a 27% drop in MGF (P < 0.05), (fig1 A). The MDF of FDI decreased, while its RMS increased suggesting fatigue. In addition, the FDS, FCU, and FCR also exhibited change during sIMC. ECR and BR muscles also showed change in both fatigue indices, (fig1 B). Fig1 C illustrates interactions among forelimb muscles, BR demonstrates a stronger correlation with ECR (R=0.5), as well as with FCR and FCU (R=0.45), and FCR and FDS (R=0.37) during the AF2-2 phase, as compared to AF1-1.
Discussion and conclusions: The MGF for all subjects decreased following the fatigue task, similar to previous reports1. While FDI was expected to be fatigued, the fatigue indicators for finger flexors (FDS, FCU, and FCR) and ECR also suggested them being fatigued, especially in the final epoch. Forearm muscles were coactivated throughout the fatiguing task. This preliminary study suggests that the slight alteration in the pattern of activity of the forearm muscles might contribute to the individual’s ability to maintain force output until failure during sIMC.
Keywords: Synergistic pattern, Maximal grip force, sustained isometric contraction, Coactivation