
Acute myocardial ischaemia is associated with reentrant ventricular arrhythmias, mainly ventricular fibrillation (VF). In normal rabbit hearts subjected to regional ischaemia, onset of VF was most frequently observed 12-15 mins after coronary artery occlusion (Bril et al., 1991). A calibrated snare was used to produce acute regional ischaemia and reperfusion with optical voltage recording. Rabbits were killed humanely and hearts were isolated and Langendorff perfused at 30ml/min. To study the electrical changes produced by acute local ischaemia, the hearts were stained with voltage sensitive dye RH237. Optical action potentials were recorded from a 16x16mm area of epicardium using a 16×16 element Hamamatsu photodiode array. Contraction motion artifacts were practically eliminated with blebbistatin (5µM). After occlusion of the left coronary artery, a progressive reduction in action potential duration, and slowing of upstroke and conduction velocity was observed in an area of the left ventricle anterior surface, accompanied by ECG S-T segment elevation. These effects were reversed when the coronary artery was occlusion was released. Ligation (duration 12-15mins) caused a decrease in APD50 (action potential duration at 50% repolarisation), in the zone of reduced perfusion, from 141±5.2ms to 53.3±9.3ms (mean±S.E.M., n=10 hearts, P<0.001). After ligation was reversed and full perfusion restored, APD50 returned to values slightly higher than normal (149±7.0ms, n.s.). Trise (action potential rise time from 10-90% depolarisation) increased from 7.2±1.0ms to 15.8±2.8ms (P<0.01). In the non-infarcted area of myocardium, no significant changes in APD50 (147±7.0ms vs 147±8.1ms) or Trise (6.4±0.4ms vs 8.8±1.4ms) were observed during occlusion. In 10 out of 13 hearts, alternans in both APD and T-wave shape was observed. In contrast, arrhythmias occurred during occlusion in only 2 out of 10 hearts. In both of these hearts, T-wave alternans magnitude increased after several minutes to a maximum, but then declined to an undetectable level prior to the appearance of arrhythmia. Optical action potentials, however, continued to show alternating amplitudes. Therefore it seems unlikely that repolarisation alternans is the mechanism underlying the generation of arrhythmias in this model of ischaemia. Instead, the explanation may involve conduction alternans leading to the development of conduction block in the ischaemic zone and reentry.
University of Cambridge (2008) Proc Physiol Soc 11, PC67
Poster Communications: Local ischaemia causes arrhythmias unrelated to T-wave alternans
S. Petchdee1, F. L. Burton1, G. L. Smith1
1. Institute of Biomedical and Life Sciences, University of Glasgow, Glasgow, United Kingdom.
View other abstracts by:
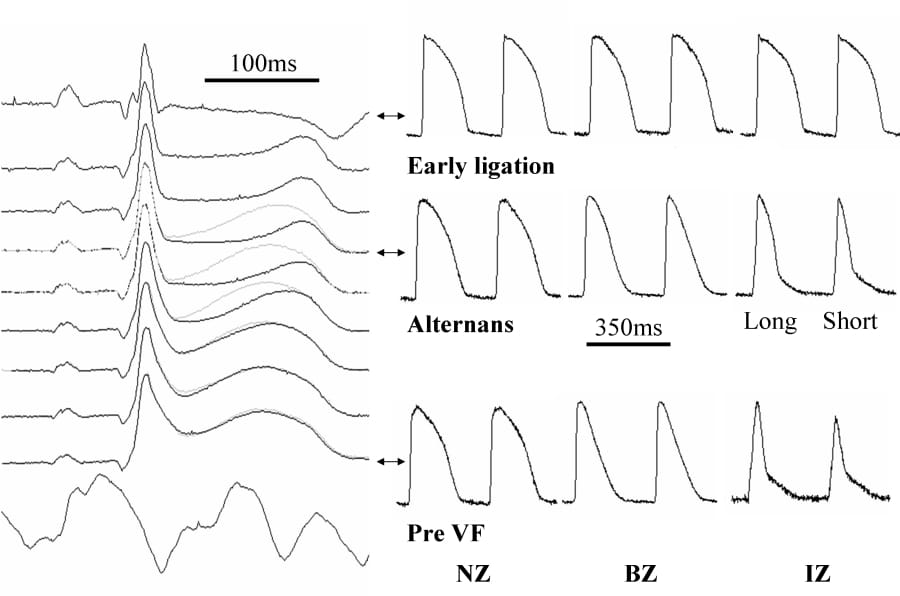
Progressive changes in ECG (left) and optical action potentials (right) following coronary artery ligation. The top trace was recorded 1min following coronary artery occlusion; the traces below represent the final 8 mins prior to VF at 14 mins. Successive ECG traces are shown in black and grey showing a 3-4min period of marked alternans. Recordings from sites in normal ‘border’ and ‘infarct’ zones (NZ BZ & IZ) are shown next to corresponding ECGs.
Where applicable, experiments conform with Society ethical requirements.