
Introduction: Peak cardiac output (Q̇peak) can be estimated non-invasively using inert gas rebreathing (IGR). IGR-derived measurements of Q̇peak are highly correlated with the gold-standard direct Fick and thermodilution methods (r≥0.94), have reasonable Bland-Altman limits of agreement with the Fick method, and may be superior to the thermodilution method during submaximal exercise in terms of reliability (1,2). There is no consensus on the optimal exercise protocol to estimate Q̇peak using IGR, which requires a rebreathing period of ~10 s as close to “maximal” effort as possible.
Aims/objectives: To compare the Q̇peak elicited by two different protocols using a non-inferiority, randomized crossover trial and considering a Q̇peak non-inferiority margin of 0.5 L/min. The comparison involved a constant load protocol modelled after peak oxygen uptake (V̇O2peak) tests that include a verification phase (Q̇CL) (3) and an incremental step protocol (Q̇step) (4).
Methods: Sample size was estimated using G*Power for a two-tailed paired t-test to detect a 0.5 effect size (Cohen’s d) at 80% power and alpha at 5%. Thirty-four participants (19 females; 25±5 y) performed two baseline V̇O2peak tests to determine peak heart rate (HRpeak) and peak work rate (Wpeak). Participants then performed the Q̇CL and Q̇step protocols on two separate occasions (four total visits) in random order. Q̇peak was measured using IGR (Innocor, COSMED, Italy). The Q̇CL protocol involved a V̇O2peak test followed 10 minutes later by cycling at 90% (Wpeak) with IGR initiated after 2 minutes. The Q̇step protocol involved a step test with IGR initiated when HR reached five beats/min below the participant’s HRpeak. We tested whether the first Q̇CL and Q̇step tests were non-inferior and estimated the reproducibility of each method (typical error; TE) with the second set of tests. Data are presented as mean±SD and between-groups confidence intervals (CI). We estimated the difference between means through a two-tailed paired t-test. To claim non-inferiority, the lower bound 95% CI of the difference between the Q̇peak exercise protocols (Q̇CL – Q̇peak) had to be within the non-inferiority margin. The project was approved by the Hamilton Integrated Research Ethics Board (13339).
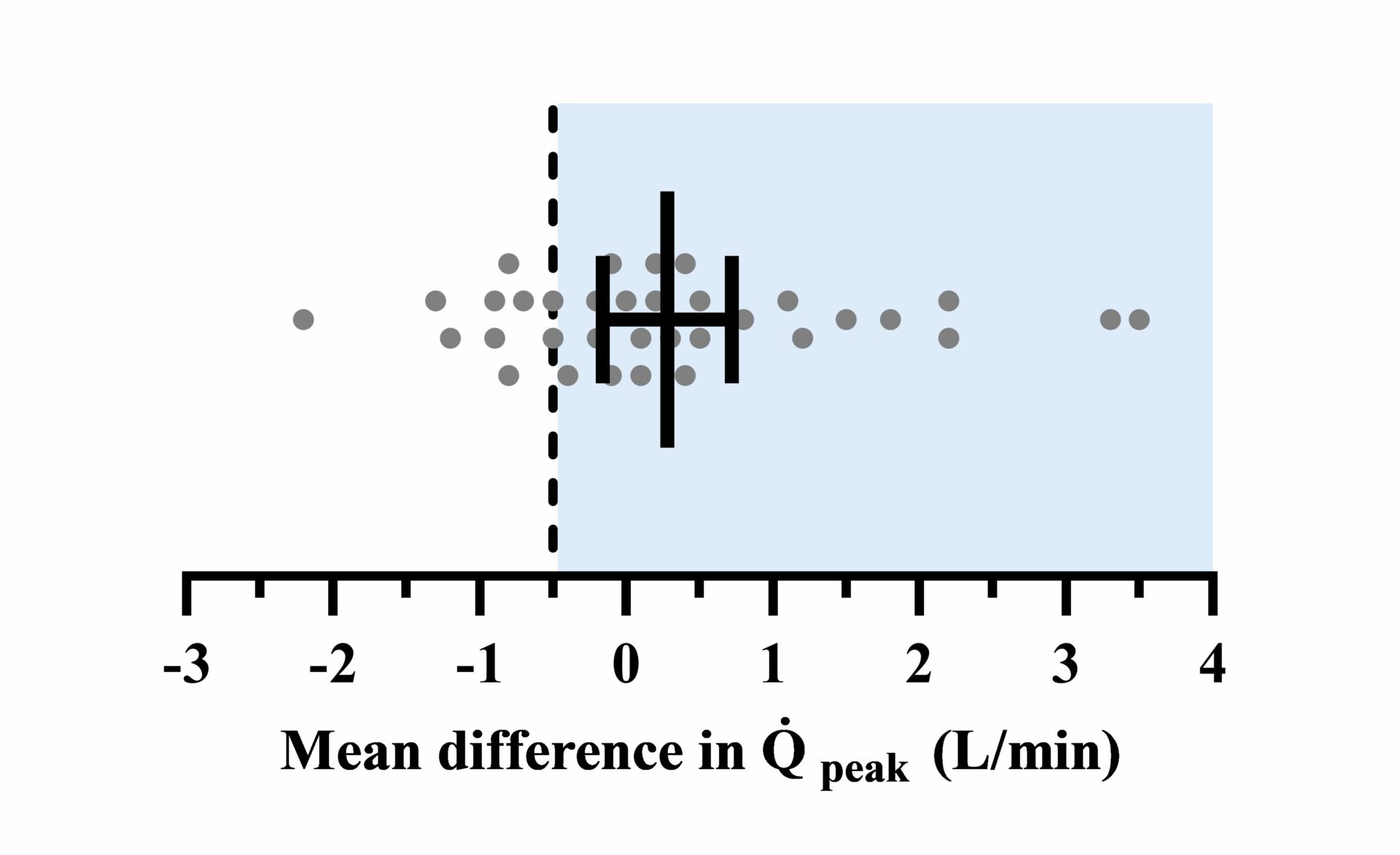
Results: The Q̇CL protocol was non-inferior to Q̇step (Q̇CL=17.1±3.2, Q̇step=16.8±3.1 L/min, p=0.20; Figure 1: 95% CI =-0.16-0.72 L/min [error bars], non-inferiority margin=0.5 L/min [dotted line]). The baseline V̇O2peak (3.13±0.83 L/min) was achieved during both the Q̇CL (3.12±0.72 L/min, p=0.87) and Q̇step protocols (3.12±0.80 L/min, p=0.82). The TE in Q̇peak was 6.6% for the Q̇CL protocol and 8.3% for the Q̇step protocol and did not differ between retesting (p=0.43 and p=0.12, respectively).
Conclusion: The Q̇CL protocol was non-inferior to the Q̇step protocol to estimate Q̇peak. Both protocols elicited V̇O2 values that were comparable to those obtained at the end of a ramp V̇O2peak test, indicating both protocols elicit a near-maximal exercise response. We conclude that both protocols are feasible and appropriate to determine Q̇peak. The Q̇CL protocol may be more convenient because it allows for the measurement of Q̇peak during the same session used to determine V̇O2peak. This may reduce participant and experimenter burden, e.g., the number of laboratory visits required.
Biomedical Basis of Elite Performance 2022 (University of Nottingham, UK) (2022) Proc Physiol Soc 49, PC07
Poster Communications: Peak cardiac output determined using inert gas rebreathing: A comparison of two exercise protocols using a non-inferiority, randomized crossover design
William Bostad1, Devin McCarthy1, Lucas Helal2, Douglas Richards3, Martin Gibala1
1 Department of Kinesiology, McMaster University 2 Hospital de Clinicas 3 Department of Medicine, McMaster University
View other abstracts by:
Where applicable, experiments conform with Society ethical requirements.