Objectives:
Chronic exposure to hypobaric hypoxia during pregnancy is associated with low birthweight and suppression of electron transfer system (ETS) proteins in placental mitochondria. Some resistance to growth restriction is seen in native high-altitude populations, which may be associated with placental metabolic changes protecting infant growth. It remains unclear whether such alterations in placental metabolism occur in intrauterine growth restriction (IUGR) pregnancies in highland Andeans at altitude. This study aimed to determine the relationship between fetal growth and placental mitochondrial respiration and enzyme activity in highland Andeans at high altitudes.
Methods:
Placental tissue and umbilical cord blood were collected from 50 Andean maternal-infant pairs living in La Paz, Bolivia (~3850m) after scheduled Cesarean delivery. Within this cohort, 26 had infants that were diagnosed with IUGR on prenatal ultrasound and the other 24 had infants of normal growth. Placental tissue was cryopreserved and analyzed using high-resolution respirometry and a substrate-uncoupler-inhibitor titration to assess for oxidative phosphorylation (OXPHOS) and ETS capacity supported by Complexes I, II, and IV. Spectrophotometric enzyme activity assays (EAAs) were used to measure citrate synthase, hydroxyacyl-CoA dehydrogenase (HOAD), lactate dehydrogenase, and hexokinase activities. Respiratory states and EAAs between groups were compared with a Student’s t-test and contextualized with clinical data through simple linear regression or one-way ANOVA. These studies were approved by the University of Colorado IRB (Approval No. 14–2178 and 17-1529) and the Ethics Review Boards for the Caja Nacional de Salud and Hospital Materno-Infantil in La Paz, Bolivia.
Results:
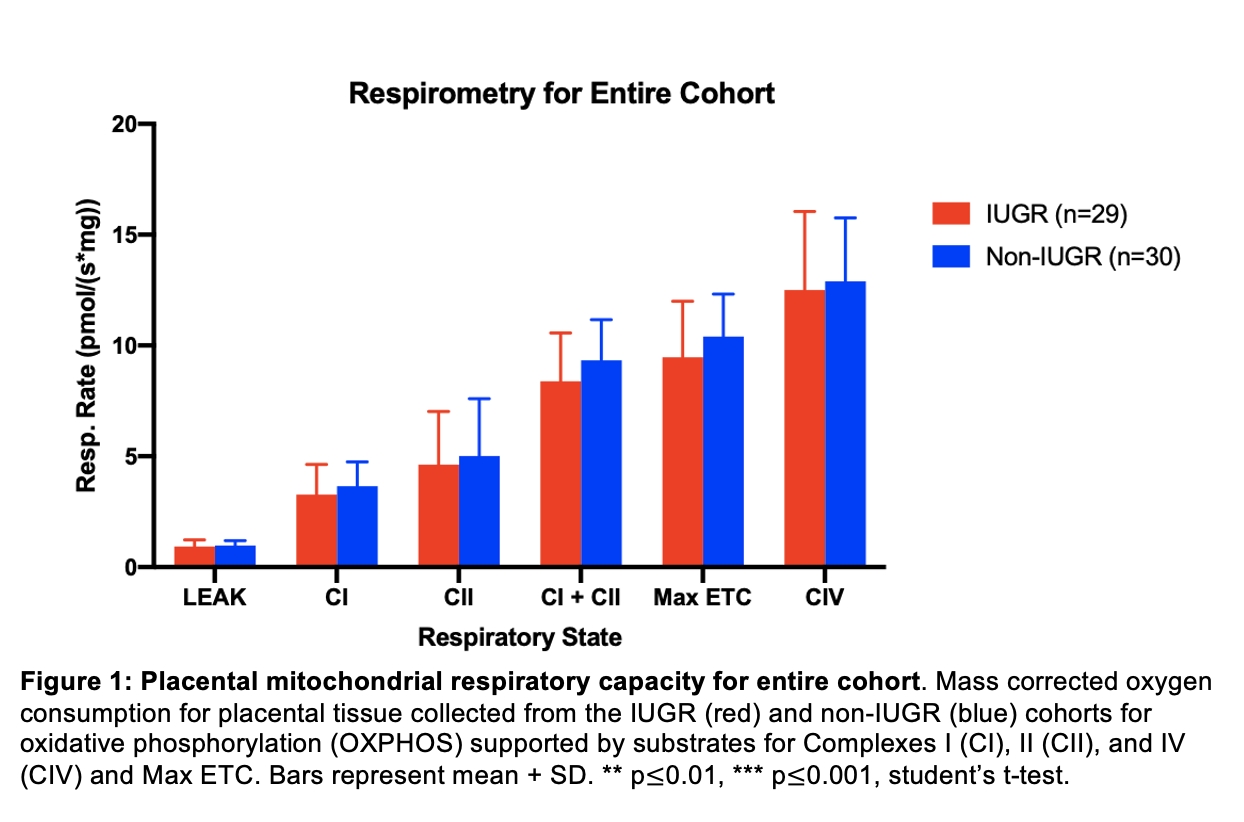
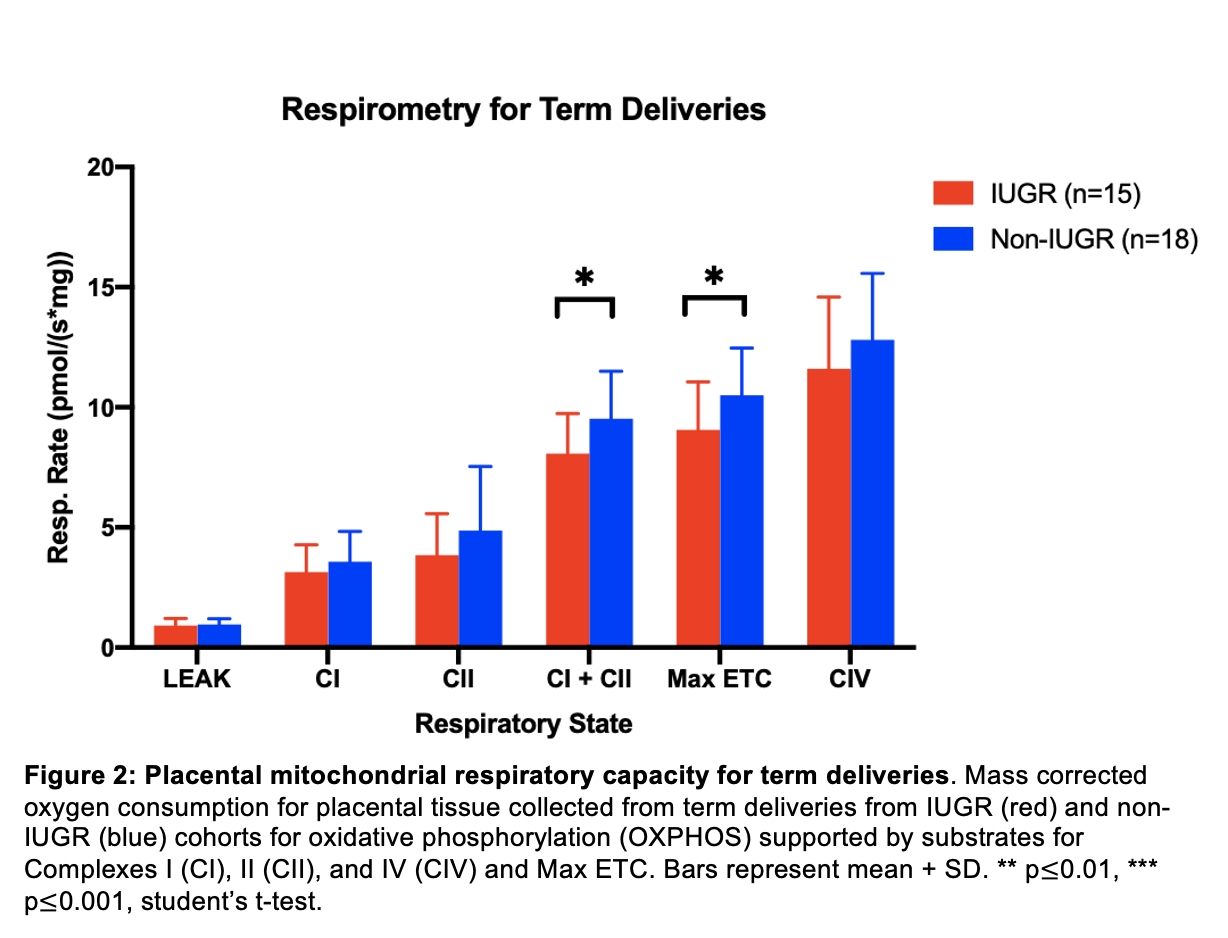
There was no significant difference in mass-specific respiratory capacity in placentas from IUGR and non-IUGR infants in LEAK state, Complex I, Complex II, or Complex IV supported respiration (Figure 1). However, when only term pregnancies were considered, maximal respiratory capacity supported by substrates for Complexes I+II and max ETC were lower (p<0.05) in the IUGR cohort (Figure 2). The IUGR placentas also had a 34.5% smaller surface area (p<0.01). Although the umbilical vein PO2 did not differ by IUGR status, the change in arteriovenous O2 difference (v-aO2) between umbilical vein and artery was 56.1% larger (p<0.01) in the IUGR cohort when corrected for infant birthweight. Cord blood hemoglobin (p<0.05), hematocrit (p<0.05), and red blood cells (p<0.05) were also higher in the IUGR cohort. There was no significant difference in the activity of any enzyme measured.
Conclusions:
Within highland Andeans at altitude, there was a mild suppression of mass-specific oxidative phosphorylation in the placenta from IUGR pregnancies, and smaller placental surface areas. The mitochondrial suppression may conserve oxygen and thereby compensate for the reduced surface area for gas/nutrient exchange in the IUGR cohort. It is possible that the influence of altitude or pre-term status has masked the full effect of metabolic changes in IUGR pregnancies. The elevated change in v-aO2 per birthweight in the IUGR cohort suggests a fetal hypoxia response despite a similar PO2 in the umbilical vein.