
Common findings after anterior cruciate ligament reconstruction (ACLR) are quadriceps muscle weakness, pain and effusion. Reduced voluntary activation may play a role, where activation is defined as an inability to recruit all motor units to a maximum level during a maximum voluntary contraction (MVC) (Rutherford et al. 1986). Determination of the median frequency of the surface electromyographic (EMG) signal has been used to estimate motor unit firing frequencies (Stulen & De Luca 1981). With ethical approval and informed consent, we examined the relationship between the median frequency of firing of surface electromyographic (EMG) recordings one and three months after surgery. Thirty one patients (25 male (M), 6 female (F)) recovering from ACLR: mean(SD) aged 30(8) years, body mass 76(9) kg, height 1.75(0.10) m took part in this study and were tested 1 and 3 months after surgery. Five recreationally active subjects (2M, 3F) aged 28(3) years, height 1.69(0.1) m, body mass 65(11) kg acted as controls. Muscle function tests included twitch superimposition and Fast Fourier transformation of surface electromyographic (EMG) recordings (5,000 cycles per second, filter 10-250 Hz) during 5s MVC to determine median frequency of motor unit action potentials of rectus femoris at 100%, 75%, 50% and 25% of MVC. Knee pain was measured using a visual analogue scale. ANOVA and post-hoc paired t tests were used to test for differences. Results are reported as means (S.E.M.) One month after surgery, a significant correlation (r=0.67, P<0.01, n=31) was found between the level of activation and strength of injured knee extensors. By 3 months post surgery, most patients (n=27) had achieved full activation but still had muscle weakness (ratio injured/uninjured I/U limb 61(3)%, MVC 127(10) Nm, 202(11) Nm, P<0.0001); the four patients demonstrating incomplete activation reported no pain. At 1 and 3 months post surgery, the EMG median frequency was significantly lower (P<0.05) in the injured compared to the uninjured limb except for 25% MVC (Fig 1); EMG amplitude was significantly (P<0.05) lower in the involved compared to the uninvolved quadriceps. Our results showed improvement in volitional activation of the quadriceps and lowered rates of motor unit firing 3 months after ACLR suggesting changes in patterns of activation and in the recruitment patterns of Type 11b fast contracting muscle fibres.
King's College London (2005) J Physiol 565P, C101
Communications: Quadriceps femoris activation and EMG median frequency after knee surgery
Drechsler, Wendy I; Cramp, Mary C; Scott, Oona M;
1. Health & Bioscience, University of East London, London, United Kingdom.
View other abstracts by:
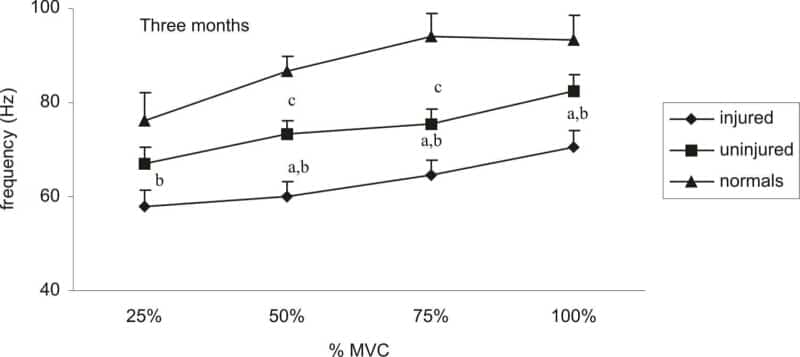
Figure 1. EMG median frequencies injured (I) and uninjured limbs (U) (n=22) three months after ACL reconstruction and average median frequencies of limbs of 5 normal (N) subjects (n=10) Means SEM a=p<0.05 I and U b=p<0.05 I and N c=p<0.05 U and N.
Where applicable, experiments conform with Society ethical requirements.