The non-baroreceptor mediated reduction in limb blood flow during local negative pressure has been attributed to the myogenic response (Lott et al., 2002). However, local negative pressure influences vascular transmural pressure, which is the stimulus underlying both the myogenic response and the venoarteriolar reflex (VAR). Venoarteriolar reflex and myogenic response mechanisms can be differentially manipulated using either venous congestion, which engages only the VAR but reduces regional perfusion pressure, or limb dependency, which engages both the VAR and myogenic response while preserving perfusion pressure (Okazaki et al., 2005). Although there may be some neural mediation of the myogenic response (Scotland et al., 2004), the VAR is entirely axon dependent, therefore topical anaesthetic block combined with the experimental manipulations described previously can separate the relative contributions of the two responses (Okazaki et al., 2005). By combining these experimental manipulations, we aimed to investigate whether the VAR contributes to vasoconstriction during negative pressure and if so, what proportion it may account for.
Following ethical approval and provision of informed consent, 25 healthy participants were recruited (14 males, 11 females; age: 32±8 y; height: 1.75±0.09 m; weight: 70.8±13.6 kg). First (n=17), we investigated the change in skin blood flux (Laser doppler fluxometry; Periflux 4001; Perimed, Järfälla, Sweden) during -40 mmHg negative pressure (180-sec), in a region of anaesthetised skin upon one lower leg (EMLA cream; Aspen pharma, Dublin, Ireland). The contralateral leg underwent the same interventions without anaesthetic block. Among a subset of participants (n=11), using methods based on Okazaki et al. (2005), the responses in skin blood flux following venous congestion (40 mmHg thigh cuff) were compared to limb dependency (45cm below horizontal), and negative pressure (-40 mmHg). The difference between the reduction in skin flux under control and blocked conditions was calculated and assumed to represent the VAR alone during venous congestion (DeltaC), and a combination of the VAR and myogenic response during limb dependency (DeltaD) or negative pressure (DeltaNP). Thereafter, assuming similar transmural stresses during each manipulation, the relative contribution of the VAR during limb dependency was estimated as [DeltaC/DD] x 100, and during negative pressure as [DeltaC/DNP] x 100. Data were analysed using repeated measures ANOVA, or Wilcoxon signed rank tests (mean ± SD or median [IQR]; p<0.05).
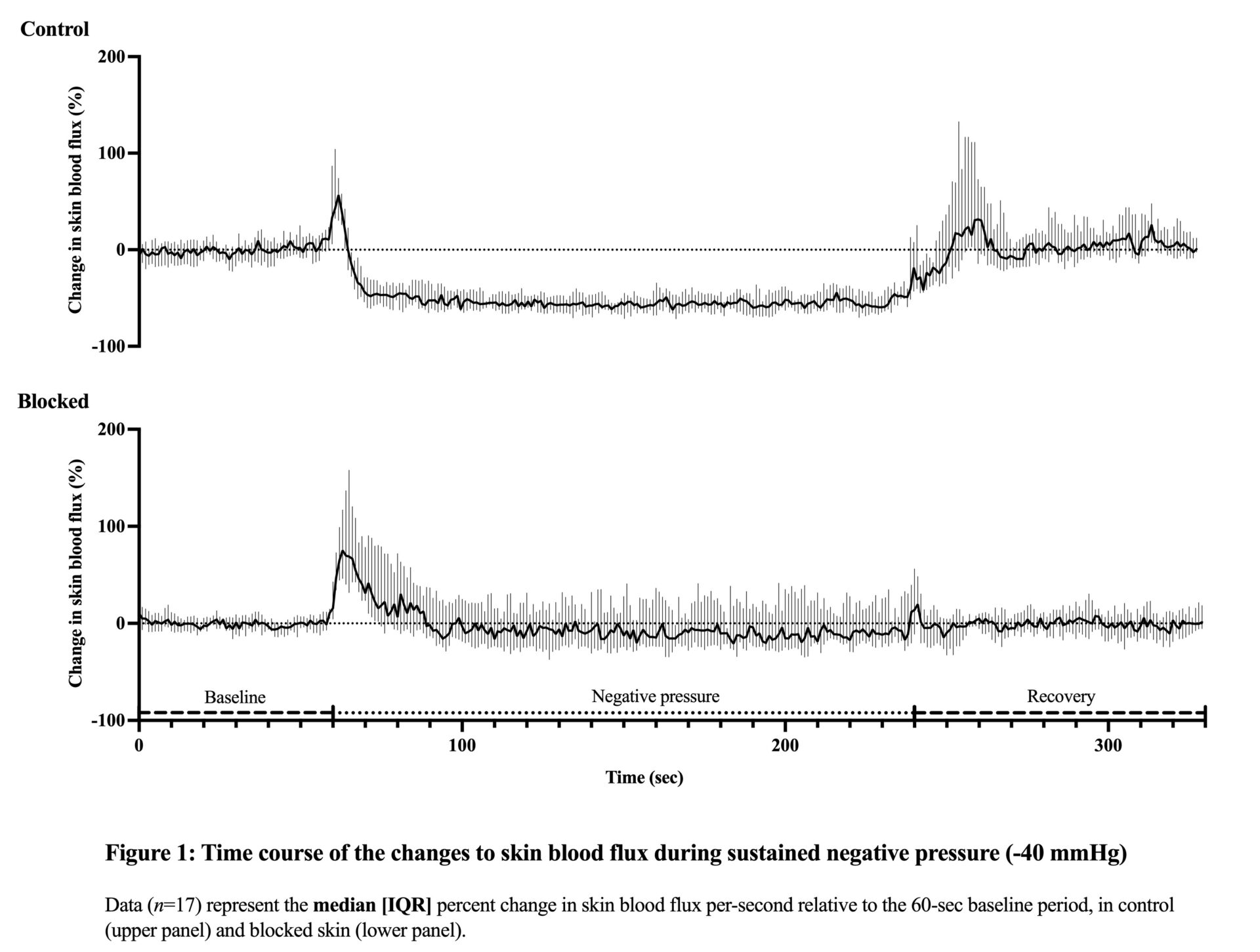
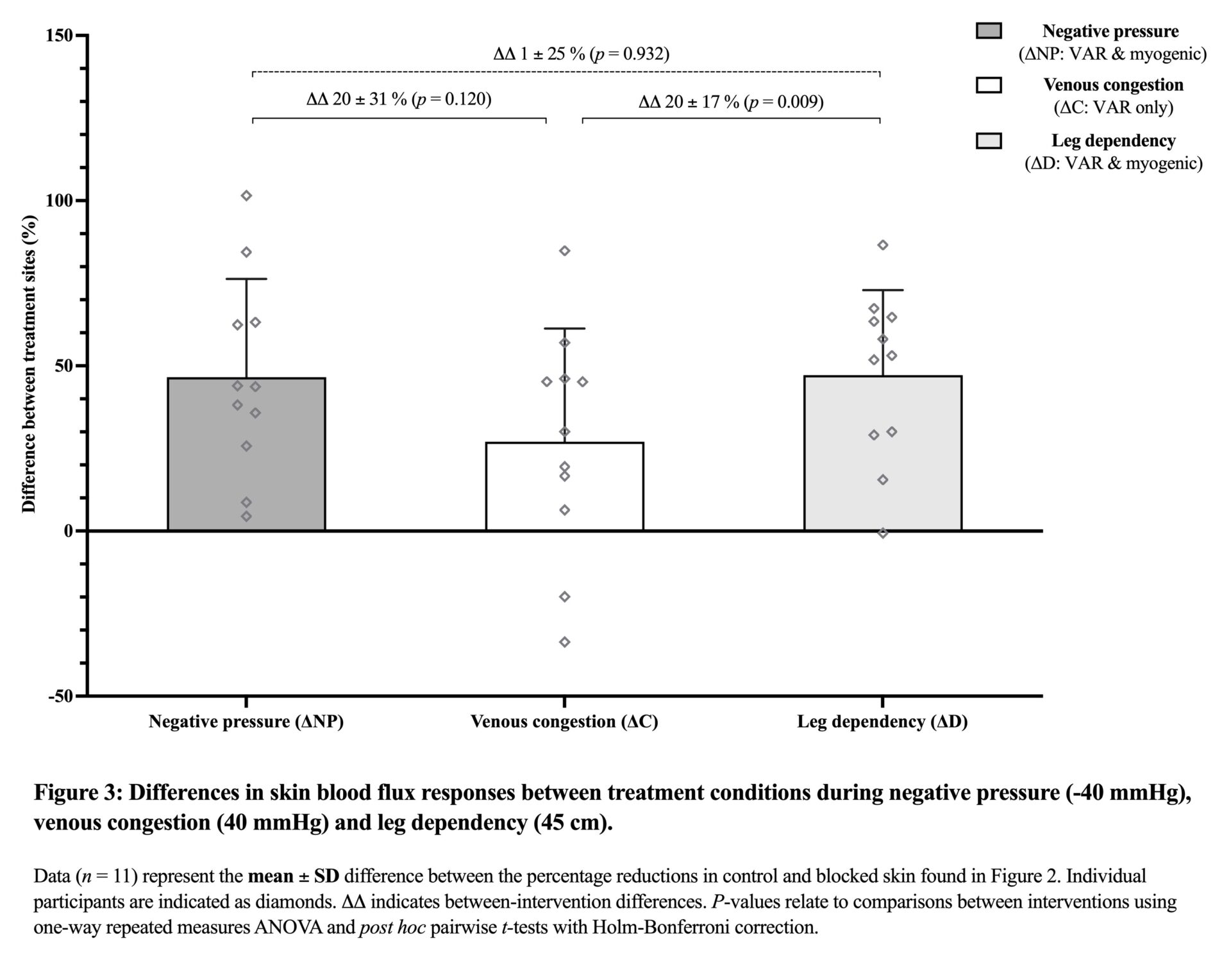
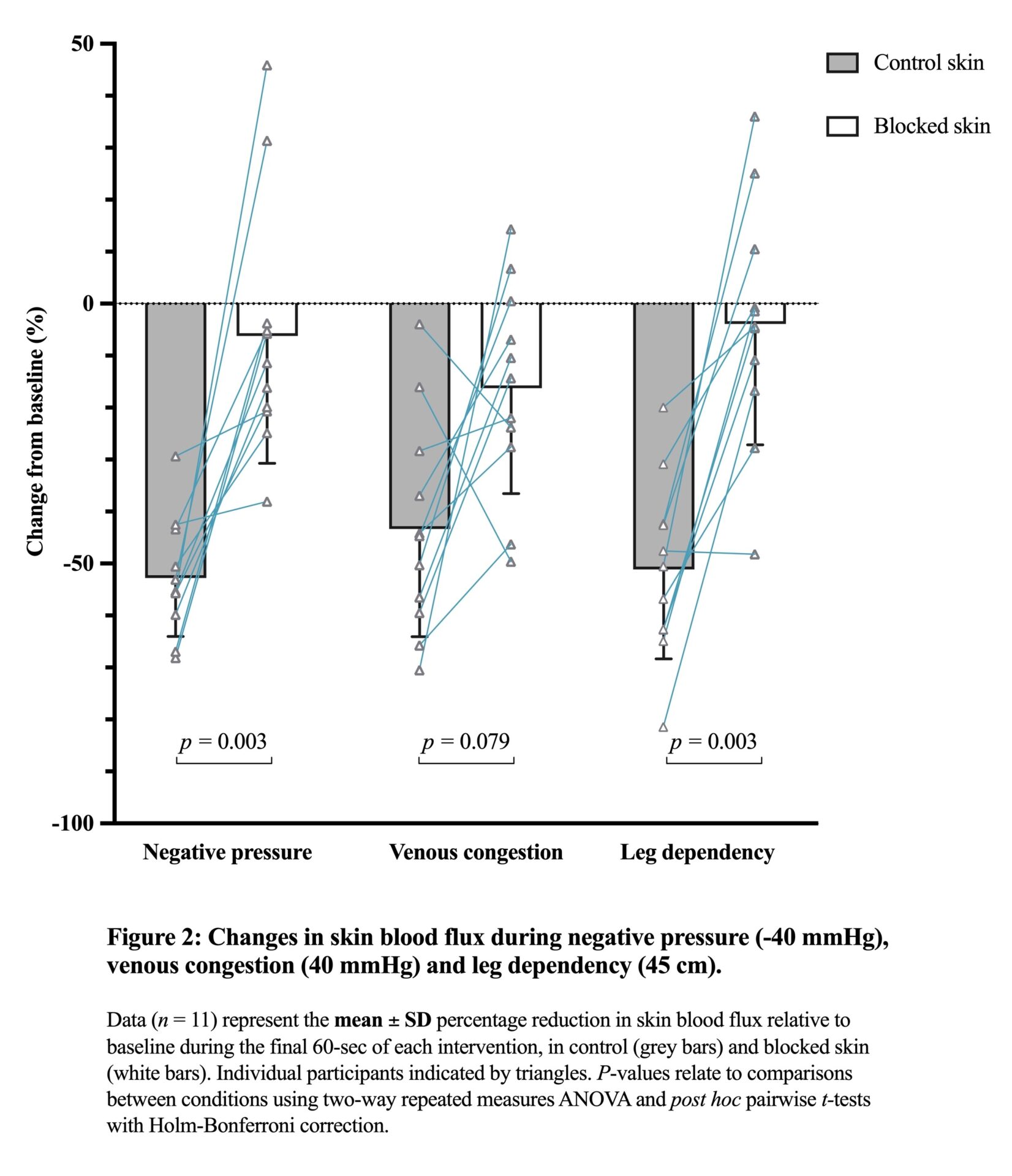
Topical anaesthetic block attenuated the reduction in skin blood flux during negative pressure (control: -53 [16], blocked: -6 [38]%, p<0.001; Figure 1). Negative pressure and limb dependency elicited similar reductions in skin blood flux (Figure 2). Results comparing the proportions of differences between skin sites (Figure 3) and between the interventions suggest the VAR is responsible for ~57% of the local vasoconstriction observed during negative pressure or limb dependency, with the remaining ~43% contributed by myogenic mechanisms.
These data suggest that the VAR does contribute to reduced skin blood flux during negative pressure, accounting for over half of local vasoconstriction. Negative pressure and limb dependency elicited comparable vasoconstriction, indicating that without baroreceptor-mediated input, local vascular responses are similar whether transmural stress is induced by gravity or external negative pressure.