Introduction: The placenta is a low-resistance vascular organ that provides an efficient maternal-fetal exchange system for oxygen and nutrients. The cardioselective beta1-adrenergic receptor antagonist, bisoprolol, is commonly prescribed to women with pre-existing cardiac disease to improve maternal stroke volume and cardiac output during pregnancy. Clinical evidence of decreased umbilical blood flow velocity and increased rate of low-birth-weight babies in women exposed to bisoprolol [1] raises safety concerns. Although the placenta is devoid of innervation, we hypothesised that bisoprolol may alter placental perfusion via a direct effect on beta-adrenergic receptors in isolated human placental chorionic plate arteries (CPAs).
Methods: CPAs (<500µm diameter) were dissected from biopsies of uncomplicated term placentas (N=3-5). Using wire myography, concentration-dependent effects of the non-selective beta-adrenergic receptor agonist isoprenaline (10-9-10-5M) were tested on CPAs pre-incubated with bisoprolol (10-5M and 10-4M) and pre-constricted with an EC80 dose of U-46619. Sensitivity was evaluated as the molar concentration of isoprenaline causing 50% of the maximal effect (Emax) and expressed as logarithm.
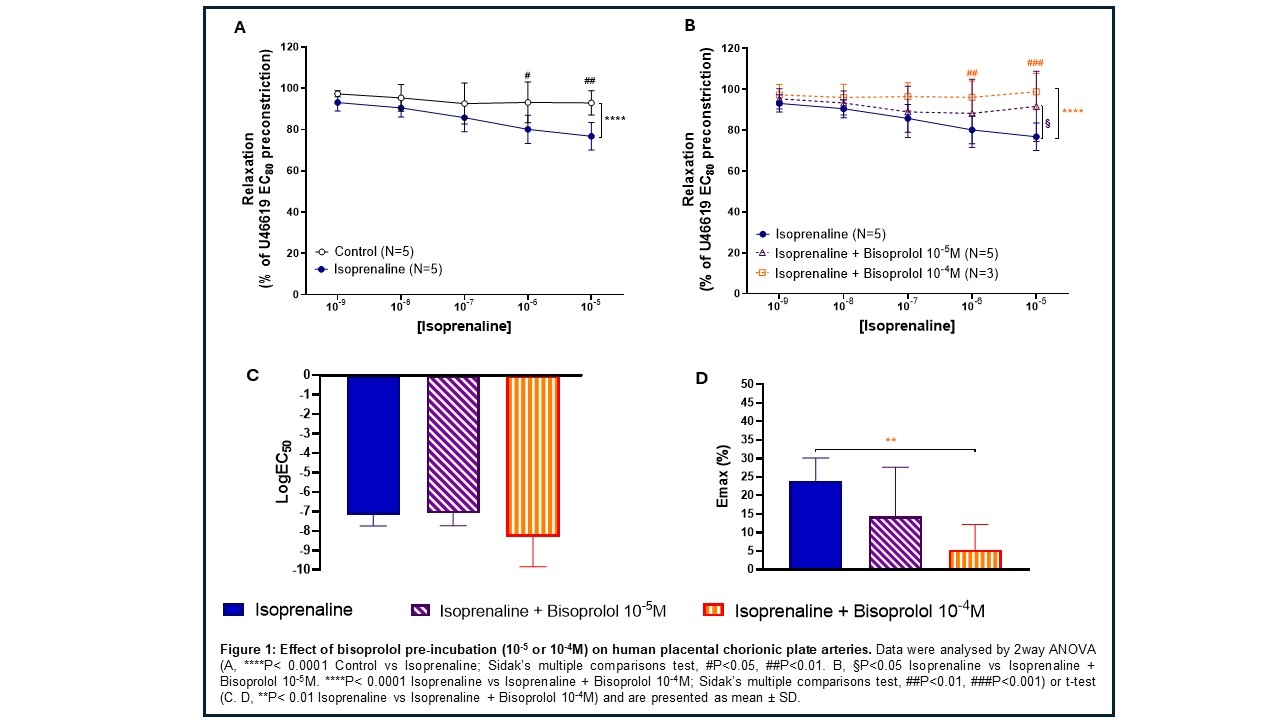
Results: Isoprenaline caused significant relaxation of CPAs in a dose-dependent manner (P<0.0001. Figure 1A). The relaxant effect of isoprenaline was significantly reduced after pre-incubation with bisoprolol 10-5M (P<0.05. Figure 1B) and was abolished by blockade with bisoprolol 10-4M (P<0.0001. Figure 1B). Maximum relaxation to isoprenaline was significantly reduced by bisoprolol 10-4M (Emax, P<0.01; 24.01 ± 6.09 vs 5.21 ± 6.94%. Figure 1C), whereas the sensitivity was not different between the two groups (P=0.800, -7.178 ± 0.56 vs -8.316 ± 1.53 LogEC50; isoprenaline vs isoprenaline + bisoprolol 10-4M).
Conclusions: These data show non-selective functional activation and inhibition of beta-adrenergic receptors on CPAs. The increased inhibitory effect of bisoprolol at supraphysiological concentration (10-4M) tested on isoprenaline-induced relaxation may suggest potential off target beta1 blockade effects. Further study is needed to determine the functional role of beta-adrenergic receptors on the fetoplacental vasculature and to identify the relationship between actions mediated by maternal plasma levels of bisoprolol on CPAs and placental perfusion.