Plasma interleukin-6 (IL-6) increases during exercise and appears dependent on factors such as exercise intensity, muscle mass recruited, and mode (concentric vs. eccentric) (for review see Febbraio & Pederson, 2002). Particularly during the later stages of prolonged endurance exercise the increase in plasma IL-6 is most pronounced. Given the late appearance of IL-6 in the plasma following prolonged exercise, there is a suggestion that the plasma IL-6 response may result from damage to skeletal muscle. A single bout of eccentric exercise produces significant muscle damage. However, the same eccentric exercise bout performed some weeks afterward does not result in damage to active muscle tissue (McHugh et al. 1999). Therefore, the aim of this experiment was to investigate the plasma IL-6 response during a single damaging eccentric exercise bout, and 5 weeks later, during another ‘repeated’ bout of eccentric exercise of the same intensity and duration, to assess the contribution of skeletal muscle damage to the IL-6 response.
Fifteen inactive male volunteers were recruited for this study. Following ethics approval and medical assessment, subjects signed informed consent documents and were randomly assigned to a concentric exercise group (CON; n = 7) or an eccentric exercise group (ECC; n = 8). Subjects performed two bouts of walking exercise separated by 5 weeks (B1 and B2) on a motor-driven treadmill at 5 km h-1 for 90 min. CON walked on the flat (0 deg decline) while ECC walked downhill on a 14 deg decline. Forearm venous samples were collected at regular intervals pre-, during and post-exercise for determination of plasma IL-6 (R&D systems ELISA kit). Maximal voluntary isometric contraction (MVC) of the quadriceps muscle group, and delayed onset muscle soreness (DOMS) were determined at the same time points, except during exercise. A 2-way ANOVA for repeated measures and Student-Newman-Keuls post hoc test were used to assess significance, with P < 0.05.
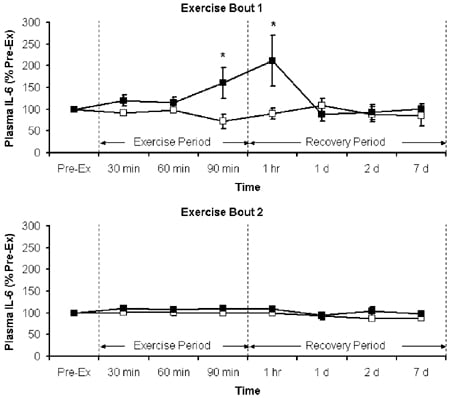
MVC and DOMS showed no muscle damage for either B1 or B2 in CON. However, there was significant muscle damage in ECC post-exercise following B1 only (not B2). Similarly, plasma IL-6 was elevated in ECC only (towards the end of B1), and peaked immediately post-exercise (Fig. 1).
In this study exercise intensity, determined by heart rate during exercise, was not different between B1 and B2 for both CON and ECC. With no muscle damage or change in plasma IL-6 following B2, the explanation for the elevated plasma IL-6 in ECC in B1 only appears entirely attributable to the increase in muscle damage reported following B1.
This work was supported by The University of Dublin, Provost Academic Development Fund.