Introduction: Eicosapentaenoic Acid (EPA) and Docosahexaenoic Acid (DHA) are Omega-3 fatty acids which have been shown to reduce the risk of cardiovascular disease in humans primarily by reducing blood pressure.
Aims: to investigate the impact of EPA and DHA on arterial pressure in healthy adults, and identify factors which may cause variation in this relationship
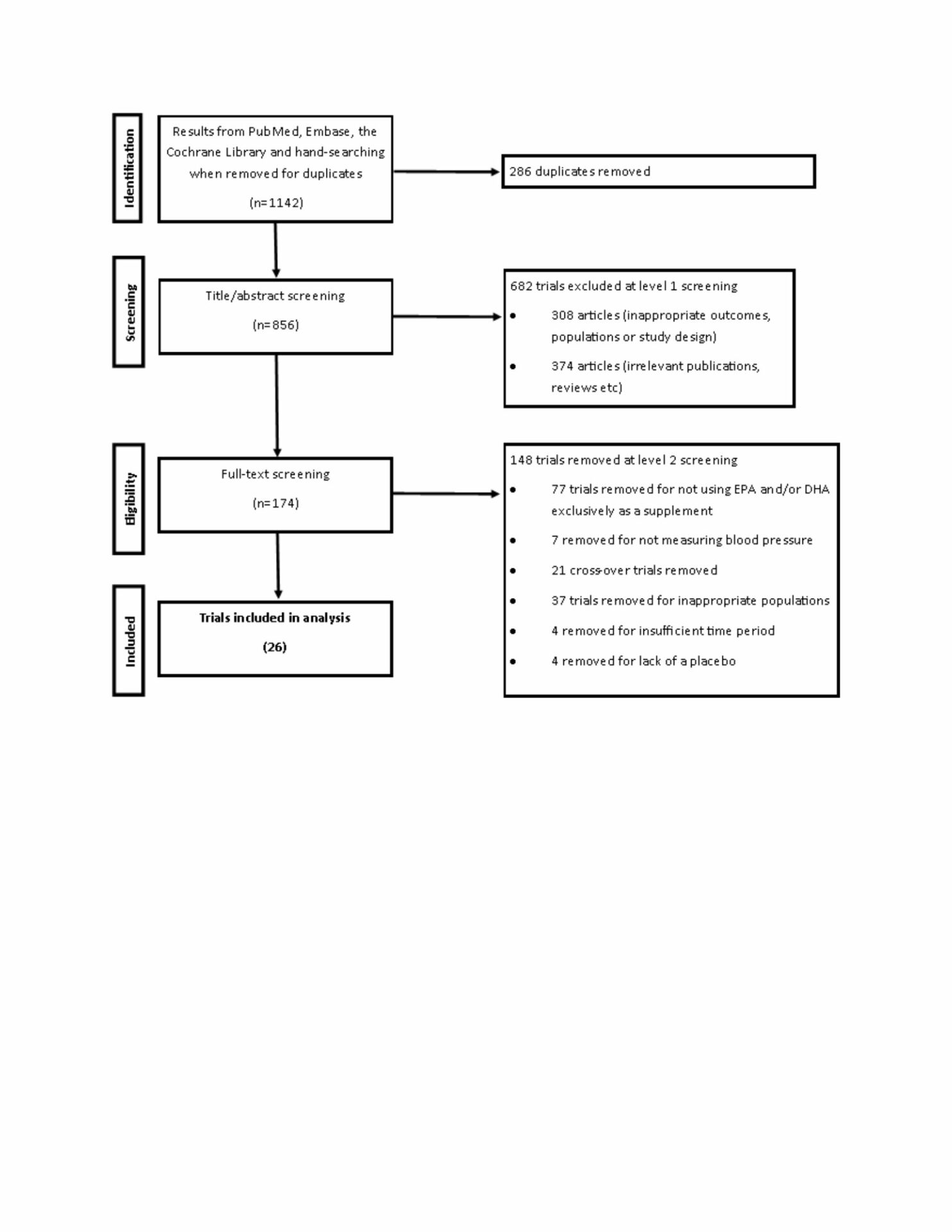
Methods: a random effects meta-analysis was carried out to establish the impact of EPA and DHA on Systolic Blood Pressure (SBP), Diastolic Blood Pressure (DBP), Mean Arterial Pressure (MAP) and Pulse Pressure (PP). A systematic search was carried out in PubMed, Embase and the Cochrane Library to identify studies which;
-
Were conducted as a single- or double-blind, randomised, placebo-controlled trial
-
Used EPA and/or DHA as a nutritional supplement
-
Lasted a minimum of 42 days
-
Used healthy adults as participants (>18 years old, and free of metabolic and cardiovascular disease with the exception of hypertension)
-
Measured SBP and DBP at both baseline and at the end of the study
On instances when data was not available from the published manuscript, a data request was made by contacting the corresponding author. Were MAP and PP were not recorded, they were calculated through the following formulas;
MAP= (SBP+DBP*2)/3
PP= SBP-DBP
All articles were dual screened by two independent researchers with disputes being resolved by a third if necessary. Bias was assessed through visual inspection of a funnel plot, followed by the performing the Cochrane RoB2 assessment on each trial.
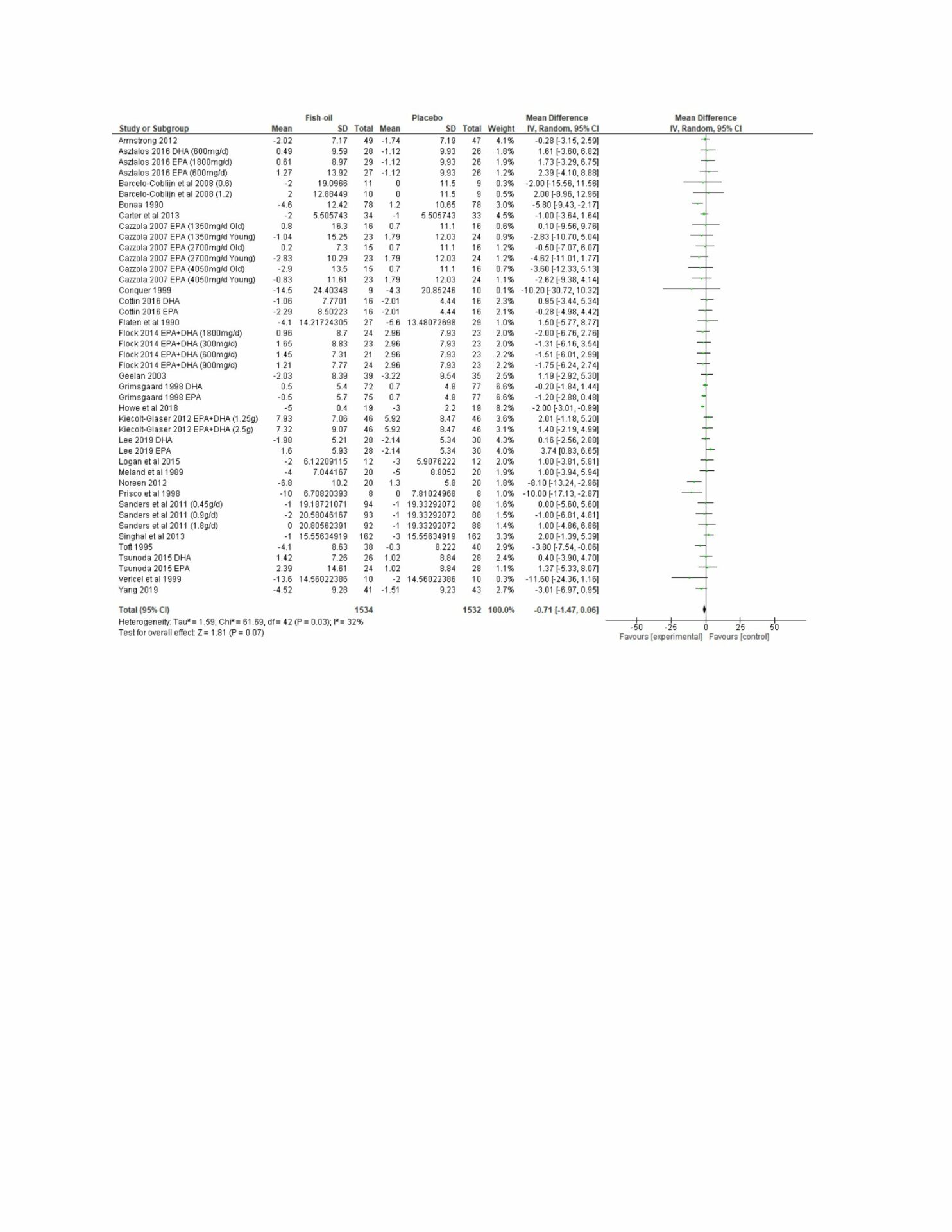
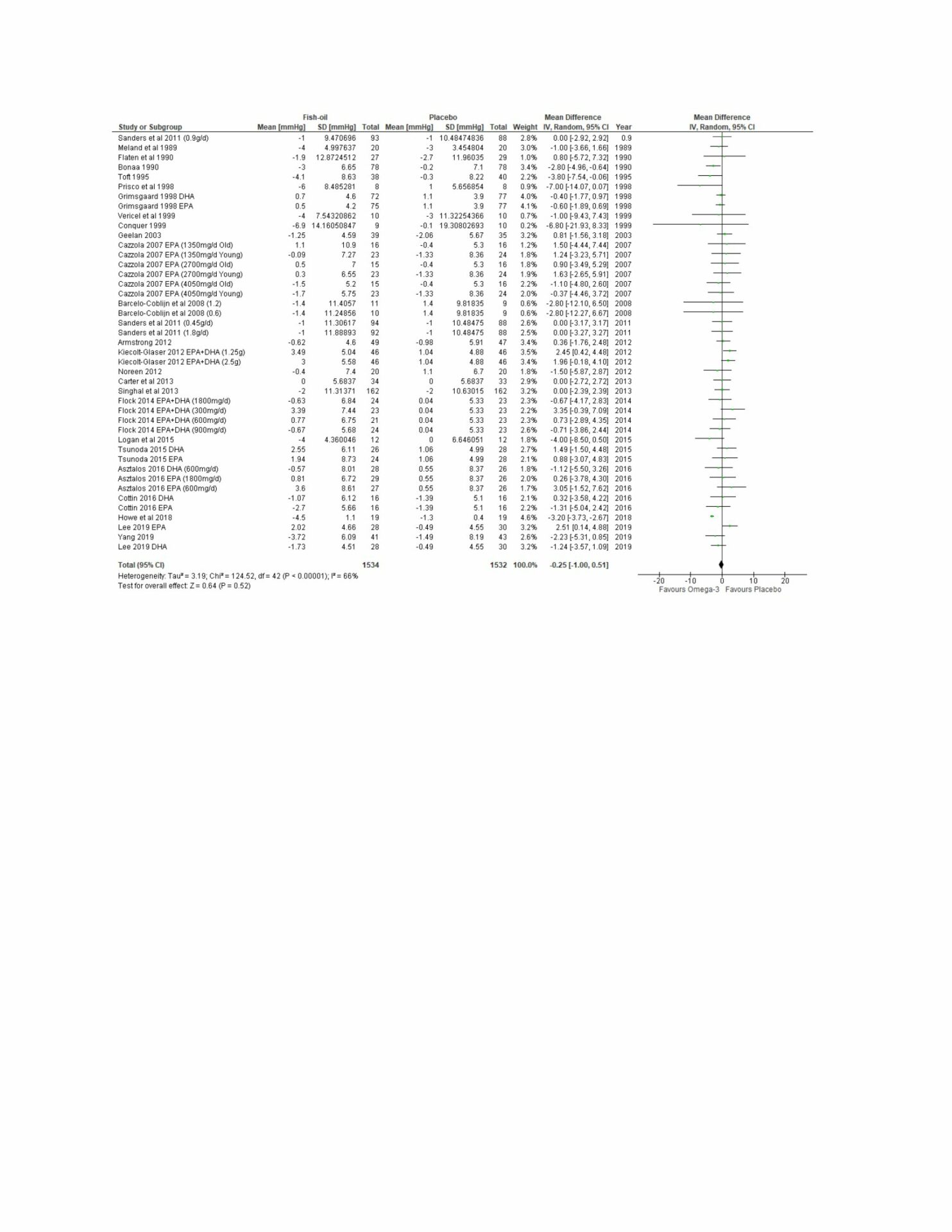
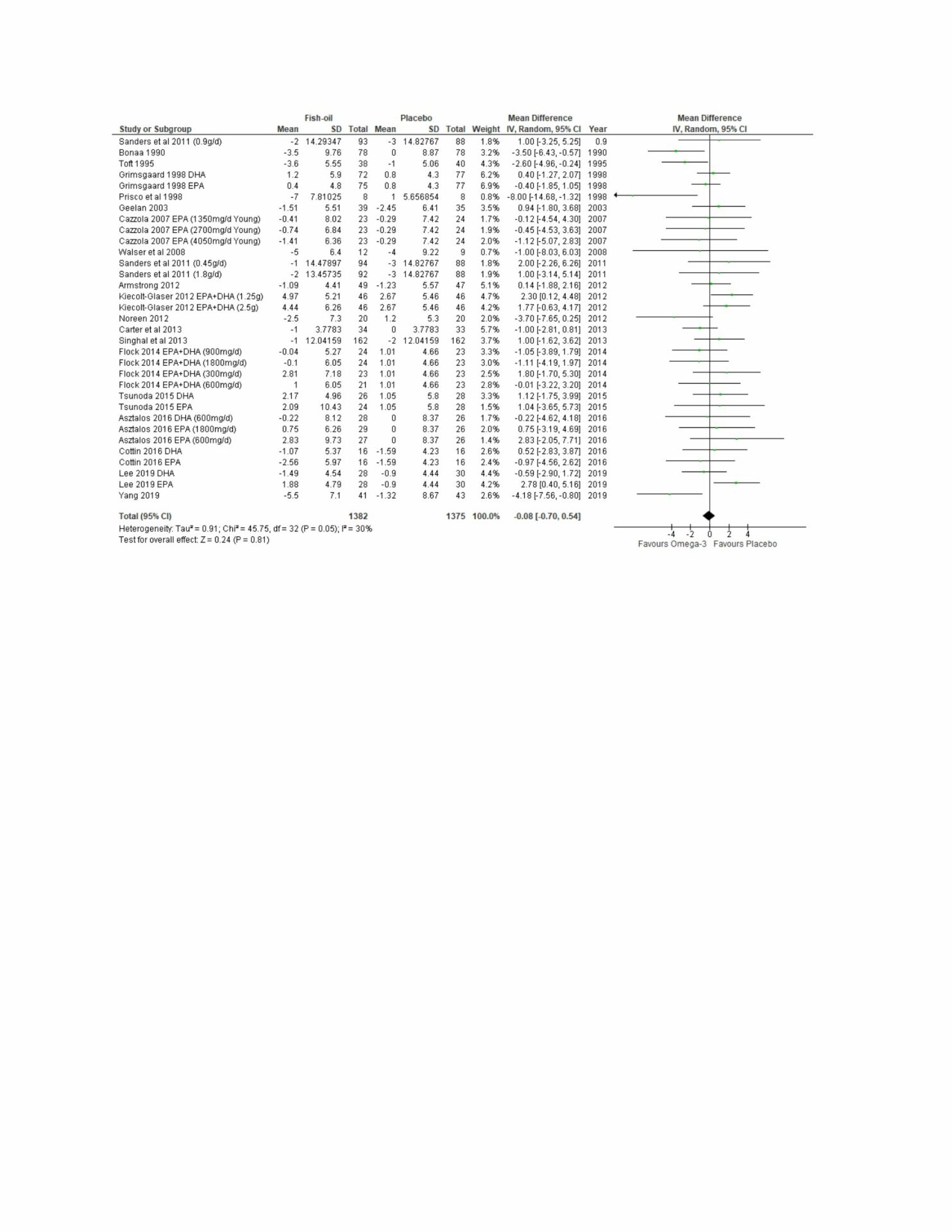
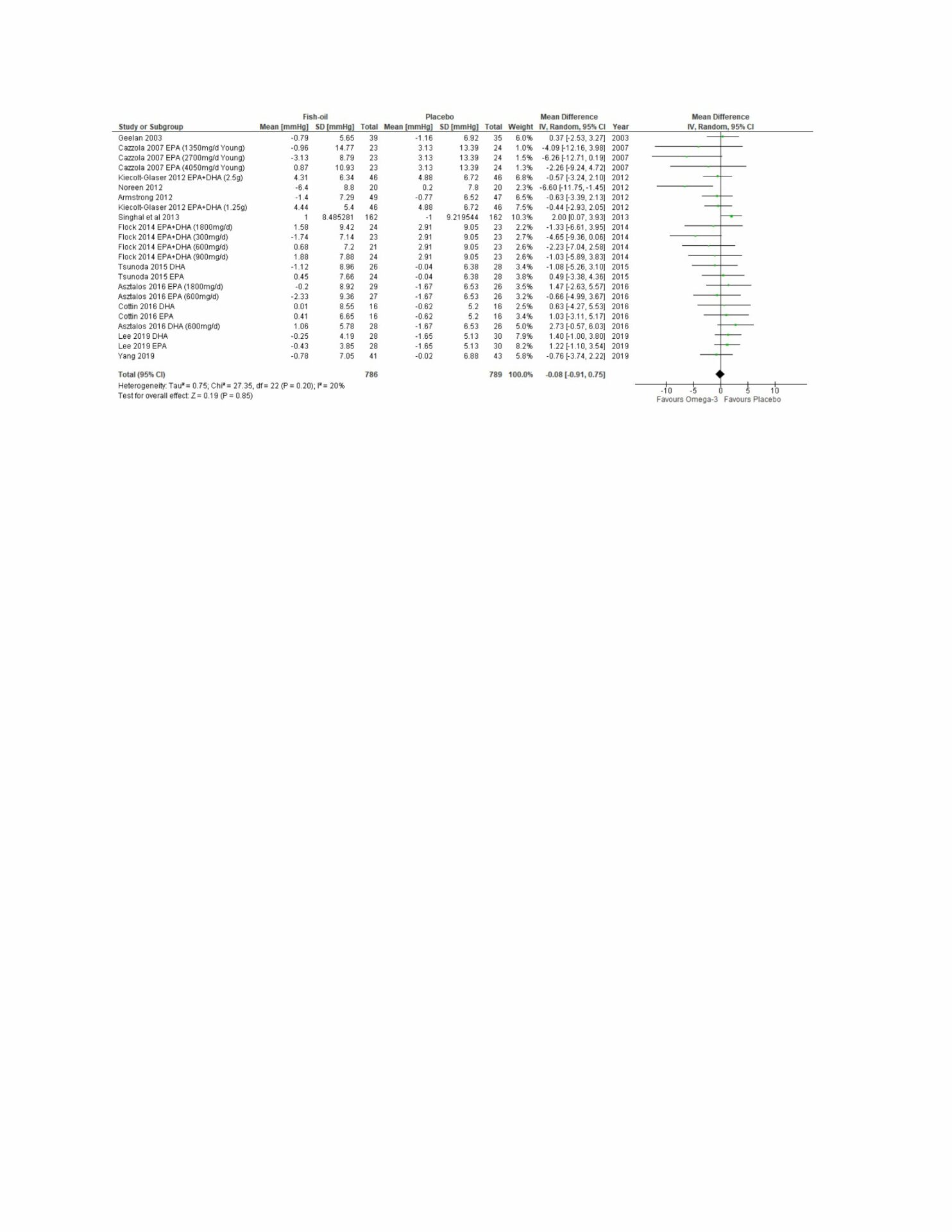
Results: a total of 26 studies were included between the years of 1989-2020 with a total of 3081 participants. There were non-significant reductions in SBP of 0.71 (95% CI’s, -1.47 to 0.06; P=0.07), DBP of 0.25mmHg (95% CI’s, -1 to 0.51; P=0.052), MAP of 0.08 (95% CI’s, -0.7 to 0.54; P=0.81) and PP of 0.08 (95% CI’s, -0.91 to 0.75: P=0.85). Subgroup analysis revealed that supplements using EPA or DHA as the predominant fatty acid had no significant impact in any of the outcomes, whereas supplements using similar concentrations of EPA and DHA had a significant reduction in SBP of 1.84 (95% CI’s, -3.11 to -0.57; P=0.004). Furthermore, studies using corn oil as a placebo were significantly more likely to show a reduction in SBP (Δ=-1.82; CI’s, -2.62 to -1.03; P<0.0001) and DBP (Δ=-1.23; 95% CI’s, -2.43 to -0.02; P=0.05).
Conclusions: as most previous meta-analyses have generally found significant reductions in blood pressure following supplementation with EPA and DHA, it is possible that the lack of significance in this study could be due to the exclusion of participants with cardiovascular or metabolic disorders. It is also possible that the exclusion of studies using dietary interventions may have had an impact. Finally, it appears that the results of studies examining the impact of EPA and DHA on arterial pressure are dependent on the ratio of EPA to DHA, as well as the placebo supplement used.