
Humans dive on full lungs because the lungs contribute largely to the O2 budget. This dependence, however, increases exposure to a range of diving risks, e.g., compression narcosis, decompression illness & hypoxia-of-ascent (HoA). Contrarian to this strategy, despite a greater-than-average lung capacity & WR-level deep diving performance capabilities, this author managed to successfully switch to the kill-proof animalesque expiration diving (ED) strategy without adversely affecting performance, suggesting O2 stores are not the be all of successful diving & that a less is more sacrificial approach may potentially offer latent performance & safety benefits.[1] Here, I report on controlled trials comparing ED vs. inspiration diving (ID) on my person & involving natural (unassisted), brief (~95 sec) & shallow (15m) dives. ED involved passive expiration to functional residual capacity (FRC) & permitted freefall; ID Involved inspiration to vital capacity (VC) & required swimming to near the bottom to overcome buoyancy; swimming was only undertaken when necessary. To ensure fatigue-free performance only six dives were performed at any one time. The following physiological parameters were measured: mean±s.d. end-dive, end-expiratory O2 gas fraction (%FEEO2; ±0.03%, Aspida, Analox), mean±s.d heart-rate (fH; Galileo/Polar Apnea, Uwatec, ±1bpm) as a proxy of systemic vascular tone, blood flow distribution & O2 consumption rate. Best-in-class outcomes are shown (Fig.1). Several major & minor mechanisms are at play to account for these paradoxical performance despite sizable differences in body O2 stores, of which the most salient are discussed. ED result in a more prompt, pronounced & sustained DR, with bradycardia persisting throughout the ascent & for some time thereafter, fortuitously, when O2 levels are at their lowest & need replenishing (Fig. 2). ED anapyrexia[2] results in enhanced blood O2 extraction at the lungs at low O2 tensions, which would slow hypoxia. Minimal lung re-inflation & inhibition of the vasodepressive pulmonary vagal inflation reflex (VPVIR), would circumvent decompression-induced hypoxia & risk of loss-of-consciousness.[3] In contrast, ID result in an anticipatory O2-consuming work response that oppose, delays & weakens the O2-conserving DR. Excessive buoyancy during descent requires taxing counter-swimming & is compounded by a relatively low efficiency stroke, resulting in rapid depletion of O2 stores. In all cases, lung re-inflation unclamps the circulation & reverses the DR, commensurate in magnitude with the absolute amount & rate of lung inflation; aggravated upon nearing the surface. Blood emenating from (warm) working muscles may further restrict the use of the lungs as an O2 source & heat-aggravate cerebral hypoxia. The ED strategy may enhance performance & safety in divers with a strong DR using a natural diving style.
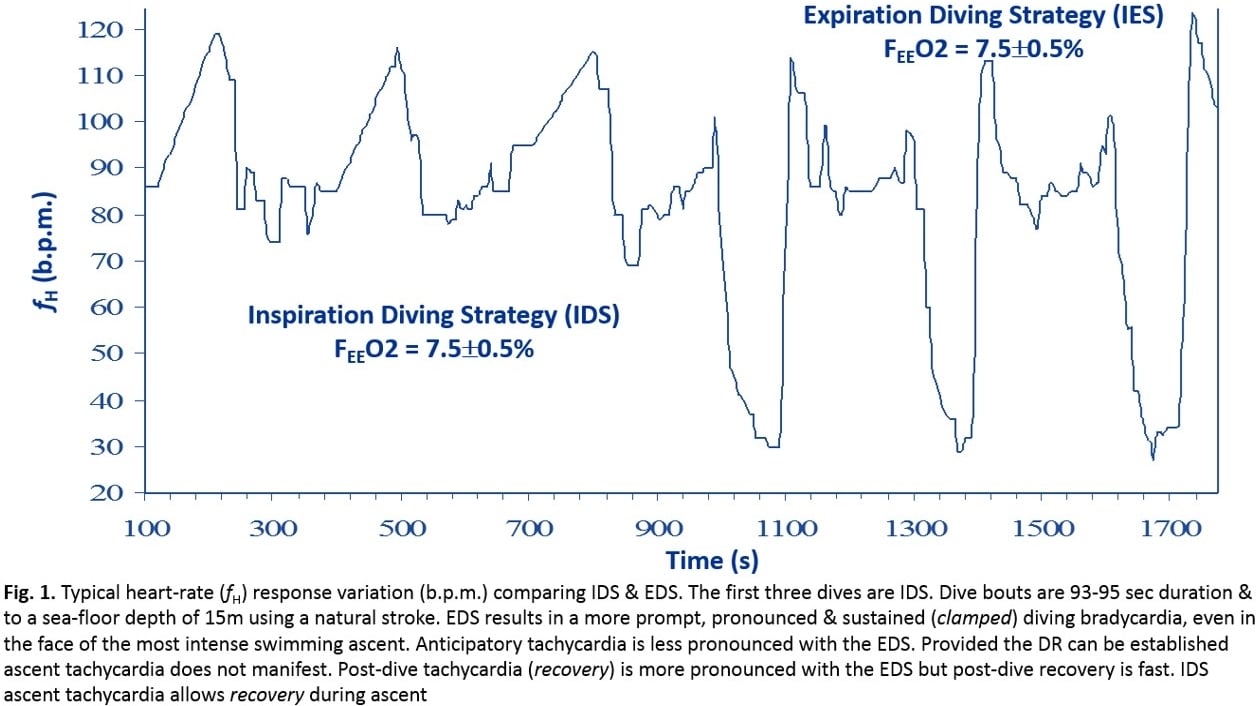
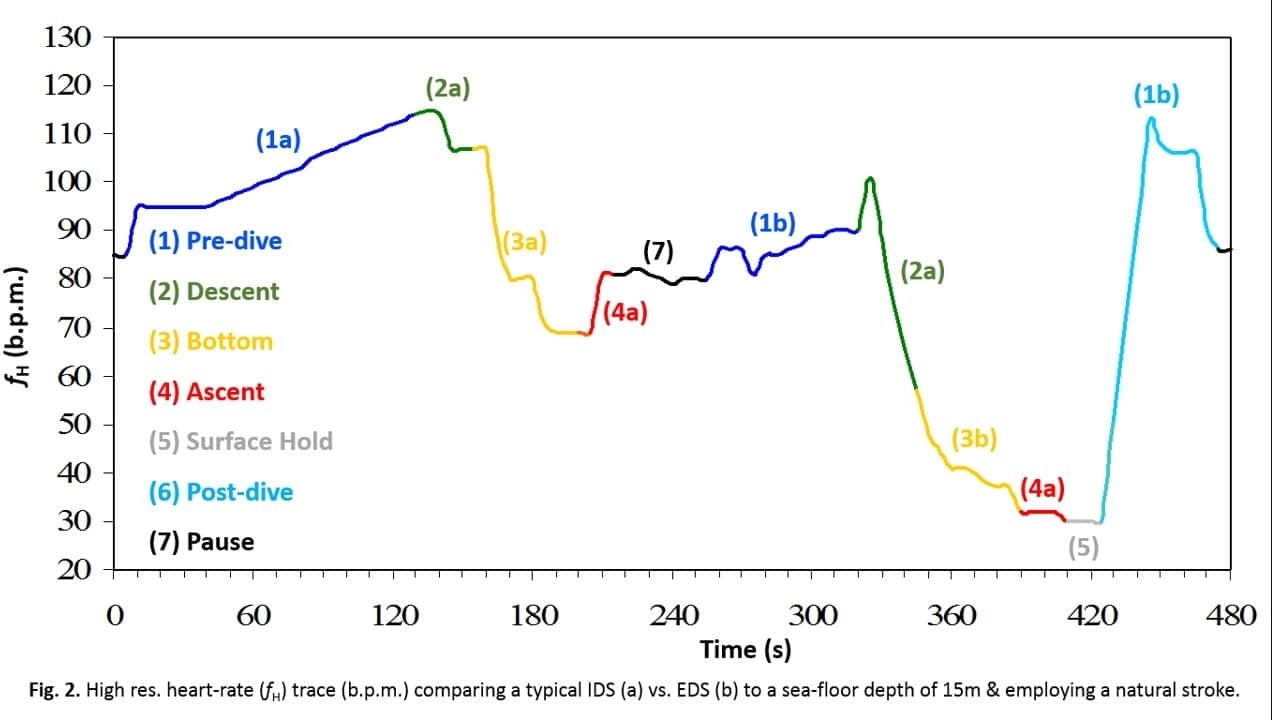
Extreme Environmental Physiology (University of Portsmouth, UK) (2019) Proc Physiol Soc 44, C25
Oral Communications: The Sacrificial Effect: Paradoxical Seal-Like Human Empty Lungs Deep Diving
S. (. Murat1
1. Bio-X Unit, Jungle Innovations, Alice Springs, South Australia, Australia.
View other abstracts by:
Where applicable, experiments conform with Society ethical requirements.