Introduction
There is increasing interest in the role of neurophysiological tools in early assessment of neurological conditions. Techniques such as transcranial magnetic stimulation (TMS) give insight into the neurophysiology underpinning functional deficits and may support improved prognostics, personalised treatment approaches and stratification for clinical trials1. TMS can be used to produce cortical maps, which give information about corticospinal drive to muscles post injury and the extent of post injury cortical reorganisation1. Being able to comprehensively map multiple upper limb muscles innervated at different spinal levels would be useful in neurological assessment, since functional tasks require synergistic use of multiple muscles and joints. This is particularly true in spinal cord injury (SCI) where differences in level and extent of damage lead to significant heterogeneity in impairments below the level of injury. Recently developed protocols allow for rapid production of cortical maps2, potentially supporting clinical use. However, these protocols still involve lengthy procedures to determine stimulation parameters (e.g. threshold) for each muscle of interest, such that producing cortical maps for multiple upper limb muscles remains time-consuming. Therefore, we investigated TMS mapping protocols which enable simultaneous mapping of multiple upper limb muscles.
Methods
Nine healthy participants and 5 people with cervical SCI participated in our pilot study. Neuro-navigated, single-pulse TMS was used with surface EMG recording to produce cortical maps for 8 upper limb muscles on one side of the body for each participant (>80 stimuli per map). For healthy participants, 2 stimulation intensities were determined, separately, for ‘distal’ and ‘proximal’ muscles. Maps for all 8 muscles were recorded at each of the 2 intensities. For participants with SCI, a single stimulation intensity was used to produce all 8 maps. Standard clinical assessments of upper limb power were also performed for participants with SCI.
Results
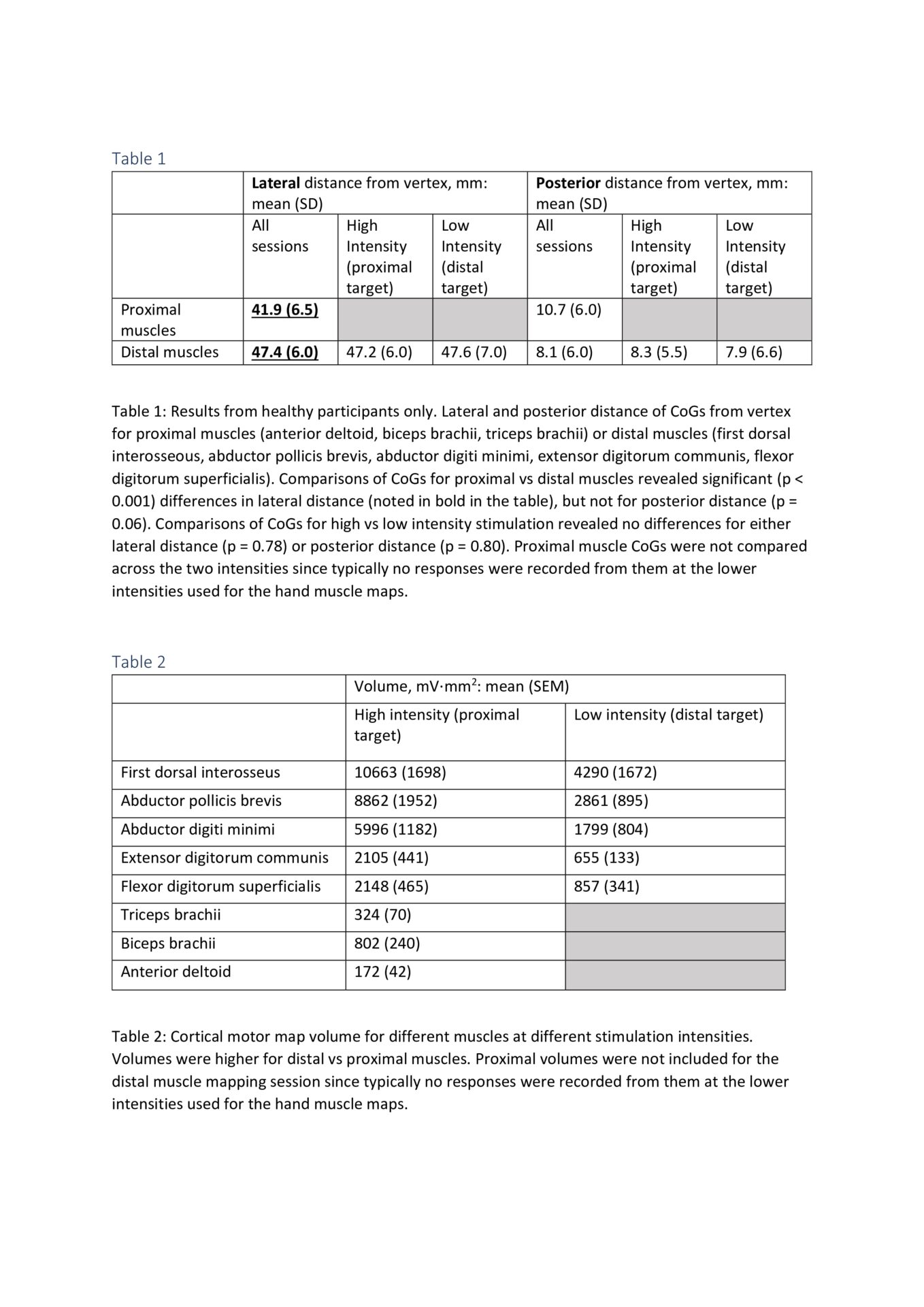
For healthy participants, somatotopic distribution of the centre of gravity (CoG) for proximal vs distal muscles was observed (see table 1). CoGs were not different between those obtained with the ‘distal’ vs ‘proximal’ stimulation intensities: CoG was preserved irrespective of stimulation intensity (see table 1). Volume of cortical map for each muscle decreased predictably from distal to proximal at both stimulation intensities (see table 2). For participants with SCI, we observed a relationship between cortical map volume for a given muscle and muscle power (r2 = 0.21, p = 0.009). As has previously been demonstrated3, somatotopic distribution of CoGs was altered in people with SCI compared with healthy participants.
Conclusion
Rapid production of cortical maps from multiple muscles simultaneously is feasible in healthy participants and in people with SCI. This method could be used to perform rapid neurophysiological assessment of the upper limb in people with cervical SCI, enabling correlation with clinical measures and potentially giving insight into recovery of function.