
Physiology News Magazine
Co-benefits of physical activity
Assisting cardiometabolic disease prevention and climate change mitigation by active travel to school
Features
Co-benefits of physical activity
Assisting cardiometabolic disease prevention and climate change mitigation by active travel to school
Features

https://doi.org/10.36866/pn.127.23
Dr Julia Zakrzewski-Fruer
University of Bedfordshire, UK
With many children and adolescents at risk of developing cardiometabolic disease (e.g. type 2 diabetes, cardiovascular disease) due to their low physical activity levels (Steene-Johannessen et al., 2020) and global concerns of climate change placing uncertainty on their futures (Gasparri et al., 2022), research on the co-benefits of physical activity for human and planetary health is highly topical and of interest to these young populations.
A recent harmonised analysis (n=47,497) reported that around two-thirds of European children and adolescents aged 2–18 years are not sufficiently active, defined as less than an average of 60 min of moderate-to-vigorous physical activity per day (WHO, 2020), when measured objectively, with higher inactivity in girls versus boys and with increasing age (Steene-Johannessen et al., 2020). Targeting young people to aid disease prevention rather than focusing efforts towards treatment in later life may also be of planetary benefit due to reduced greenhouse gas emissions associated with disease either directly via, for example, blood analysis consumables, drug manufacturing and clinical waste disposal associated with diagnosis and treatment, or indirectly via disease effects on lifestyle, among other things (Eckelman et al., 2018).
A climate change mitigation strategy
Although a universally accepted, detailed definition is lacking (Saunders et al., 2013), “active travel” to school is often assessed according to the number of days walking, cycling or scootering to school across the week and represents a key opportunity for engaging in health-enhancing physical activity among young people. Simultaneously, active travel reduces the reliance of young people on using carbon-consuming transport modalities and, thereby, over time, can help to mitigate the rate and severity of climate change. From a public health perspective, encouraging active travel to school may be a feasible approach to increasing physical activity levels at the population level because, unlike many opportunities for physical activity, transport is typically a necessity of everyday life with almost all young people travelling to school on five days per week across the school year. Further, the transport characteristics (e.g. mode and intensity of the physical activity that constitutes the active travel) and designated route are usually consistent between days, but can be amenable to change to enhance the potential health benefits. Yet, an understanding of the acute and chronic physiological responses to active travel to school is lacking. For example, insight into the intensity of the active travel through heart rate and expired air monitoring would provide a useful quantification of energy expenditure and intensity and examining the cardiometabolic responses, such as glycaemic control and insulin sensitivity, would have implications from a disease prevention perspective.
and climate change mitigation.
Healthy and sustainable modes of travel
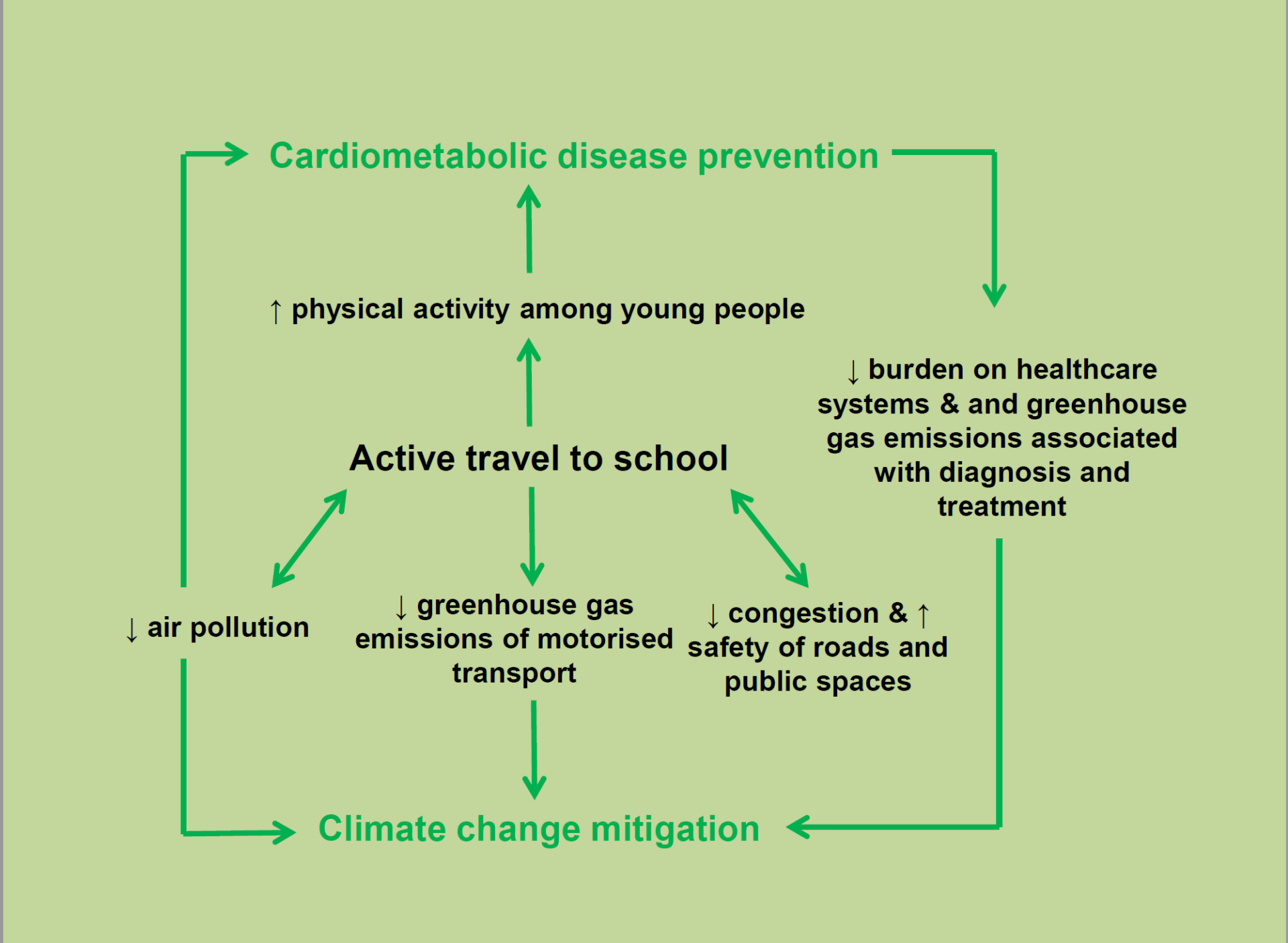
The weight of the evidence based on intervention and prospective observational studies among children and adults combined supports the positive effects of active travel over longer periods and distances on cardiometabolic health outcomes, particularly for diabetes risk (Saunders et al., 2013) (Fig.1). Although, data in young people specifically were often confined to measures of obesity (Saunders et al., 2013). In a large multinational sample of 6,797 children aged 9–11 years, active travel to school was associated with lower measures of adiposity across 12 countries representing a wide range of sociocultural variability, suggesting that this finding applies on a global scale (Sarmiento et al., 2015). Further, there is some evidence that active travel to school is associated with higher cardiorespiratory fitness among children and adolescents (Lubans et al., 2011). To draw stronger conclusions among children and adolescents specifically, further research utilising study designs from which causality might be inferred, such as randomised controlled trials, crossover trials and interventions, with measures of cardiometabolic disease other than obesity is required (Saunders et al., 2013).
Also, current literature has employed varying definitions of active travel, which poses challenges in synthesising the available evidence (Saunders et al., 2013). Indeed, accumulating evidence supports the acute benefits of single bouts of physical activity (often performed in a laboratory environment) on cardiometabolic health markers among children and adolescents, including moderating postprandial concentrations of plasma glucose, insulin and lipids for up to 24 hours (Cockcroft et al., 2015; Thackray et al., 2015).
Based on this evidence, which has typically included structured exercise, the likelihood of achieving cardiometabolic health benefits through active travel will depend on the duration, intensity (affected by the nature of the route, inclines and terrain), mode (e.g. walking, cycling, scootering) and frequency of the physical activity that characterises the active travel. Yet, it may not be possible, for example, to achieve moderate or vigorous intensities during a walk to school. As such, determining the health-enhancing physical activity characteristics specifically for feasible active travel modes, intensities and durations that can be implemented in real-life settings would help inform a health-based definition of active travel that could be used in research and practice.
Real life application of healthy active travel?
When considering application to real life, it may be more feasible for active travel to contribute to light or moderate physical activity, which will inherently reduce sedentary time. Although vigorous physical activity is likely to confer more pronounced benefits to health due to the higher rate of energy expenditure and the heightened demands on the cardiorespiratory system, it may be challenging to achieve such intensities during typical modes of active travel, such as walking to school. In certain instances, it may be possible for active commutes to reach vigorous intensities; for example, cycling on hilly routes, but such scenarios may be rare.
Further, carbon dioxide production per unit of time increases with physical activity; taking into account physical activity duration and intensity, there may be a specific physical activity intensity that is optimal in terms of the lowest gross carbon dioxide production during the active commute. Such data could help to contribute to efforts to reduce greenhouse gas emissions. Regarding the duration of the commute, five-year old children who walked to primary school were not more active across the week compared with those who were driven, perhaps because the distance to school at this age may be too short to contribute significantly to daily activity (Metcalf et al., 2004). Hence, the age of the participants may limit the duration of the active commute, which requires consideration for real-life application of possible physiological research showing benefits of longer commutes. For these younger children who require parental assistance on the commute to school, there may be an additional benefit of enhanced physical activity to the parents or caregivers.
Good for our physical and mental health
Aside from the physical activity characteristics, active travel will increase time spent outside for young people before and after school, which could improve vitamin D status through sunlight exposure, promote social interactions, confidence and self-efficacy, and enhance interactions with nature, as well as having potential knock on effects for additional physical activity, such as playing at the park during or after the commute. That said, high levels of air pollution on some commutes may negate some of the positive health effects of the physical activity, especially for children who are more susceptible than adults to the adverse health effects of air pollution due to greater physiological sensitivity and higher respiration rates (Al-Kindi et al., 2020).
Additionally, active travel may interact with other diet and physical activity-related behaviours throughout the day, such as breakfast consumption, snacking, physical activity at other times in the day, and it is unclear how such potential compensatory responses might either negate or enhance any positive effects of active travel.
The need to adopt health- and planet-friendly behaviours
Addressing the global burden of preventable cardiometabolic diseases and climate change may require similar, multidisciplinary approaches. Indeed, these two global emergencies share common characteristics, with both escalating in recent decades due to a complex interplay of modern human practices and the consequences often not being tangible or observable until serious adverse outcomes emerge (e.g. blindness with type 2 diabetes, large-scale fires due to rising temperatures). Physiological research can provide an important understanding of the acute and chronic cardiometabolic risk marker responses to active travel across different intensities, modes, durations, and frequencies to inform messages that could help to promote active travel for both health promotion and climate change mitigation (i.e. efforts to reduce or prevent emission of greenhouse gases). Additionally, research focused on adaptation (e.g. minimising the adverse consequences of climate change) will be important to promote active travel in our changing climates, including understanding thermoregulatory responses to help provide an understanding of the possible bidirectional relationship of active travel with climate change in the context of barriers and facilitators to active travel engagement. With this in mind, interdisciplinary efforts across the fields of physiology and behavioural science may be valuable in providing effective messaging based on physiological findings with the hope of increasing engagement in active travel across our communities for human and planetary health benefits. This will aid attempts from public health professionals and researchers to promote various modes of active travel as health- and planet-friendly alternatives to motorised forms of transport.
References
Al-Kindi SG et al. (2020). Environmental determinants of cardiovascular disease: lessons learned from air pollution. Nature Reviews Cardiology 17(10), 656–672. https://doi.org/10.1038/s41569-020-0371-2
Cockcroft EJ et al. (2015). High intensity interval exercise is an effective alternative to moderate intensity exercise for improving glucose tolerance and insulin sensitivity in adolescent boys. Journal of Science and Medicine in Sport 18, 720–724. https://doi.org/10.1016/j.jsams.2014.10.001
Eckelman MJ et al. (2018). Estimated global disease burden from us health care sector greenhouse gas emissions. American Journal of Public Health 108(Suppl 2), S120–S122. https://doi.org/10.2105/AJPH.2017.303846
Gasparri G et al. (2022). Climate emergency: how should COP27 do better for adolescents and young people? British Medical Journal 376, o816. https://doi.org/10.1136/bmj.o816
Lubans DR et al. (2011). The relationship between active travel to school and health-related fitness in children and adolescents: a systematic review. International Journal of Behavioral Nutrition and Physical Activity 8, 5. https://doi.org/10.1186/1479-5868-8-5
Metcalf B et al. (2004). Physical activity cost of the school run: impact on schoolchildren of being driven to school (EarlyBird22). British Medical Journal 329, 832–833. https://doi.org/10.1136/bmj.38169.688102.f71
Sarmiento OL et al. (2015). Relationships between active school transport and adiposity indicators in school-age children from low-, middle- and high income countries. International Journal of Obesity Supplements. 5(Suppl 2), S107–S114. https://doi.org/10.1038/ijosup.2015.27
Saunders LE (2013). What are the health benefits of active travel? A systematic review of trials and cohort studies. PLoS One 8(8), e69912. https://doi.org/10.1371/journal.pone.0069912
Steene-Johannessen J et al. (2020). Variations in accelerometry measured physical activity and sedentary time across Europe-harmonized analyses of 47,497 children and adolescents. International Journal of Behavioral Nutrition and Physical Activity 17, 38. https://doi.org/10.1186/s12966-020-00930-x
Thackray AE et al. (2013). Acute high-intensity interval running reduces postprandial lipemia in boys. Medicine & Science in Sports & Exercise 45, 1277–1284. https://doi.org/10.1249/mss.0b013e31828452c1
World Health Organization (2020) Guidelines for physical activity and sedentary behaviour. Geneva: World Health Organization. Available at https://www.who.int/publications/i/item/9789240015128