
Physiology News Magazine
Heart disease link to oxygen in the womb
Studies of chick embryos and babies in La Paz, the highest city in the world, are helping to uncover a link between low oxygen in the womb with fetal growth restriction and heart disease in later life
Features
Heart disease link to oxygen in the womb
Studies of chick embryos and babies in La Paz, the highest city in the world, are helping to uncover a link between low oxygen in the womb with fetal growth restriction and heart disease in later life
Features
Dino A Giussani
Department of Physiology, Development & Neuroscience, University of Cambridge, UK
https://doi.org/10.36866/pn.74.24

Prenatal origins of heart disease
Heart disease is the greatest killer in the UK today, imposing a substantial burden on the nation’s health and wealth. The concept that traditional risk factors, such as smoking and obesity, increase the risk of heart disease is familiar to all of us. However, it does little to explain why some individuals develop the disease and others do not. Hence, in addition to the genetic basis of cardio-vascular disease, a third concept has now become established – one of developmental programming. This states that a component of both the cardiovascular health we enjoy and the risk of heart disease in adult life can be predetermined before birth, not only by our genes but also by their interaction with quality of the prenatal environment. In pregnancy complicated with adverse intra-uterine conditions, physiological adaptations are enforced in the unborn child and placenta, which can reduce the growth of the fetus (*1) and alter the development of key organs and systems, such as the heart and circulation. Whilst they are necessary to maintain viable pregnancy and sustain life before birth, these adaptations come at a cost, claiming many biological trade-offs. Overwhelming evidence in humans in more than a dozen countries now links development under sub-optimal intrauterine conditions leading to low birth weight with increased rates of heart disease and its major risk factors – hypertension, atherosclerosis and diabetes (Barker, 1998).
*1: Fetus. Much controversy exists over the spelling of the word ‘fetus’. The Oxford Dictionary states that the word was adopted from the Latin noun meaning ‘offspring’ and the verb ‘feteo’ meaning ‘to breed’. Interestingly, the Latin verb ‘foeteo’ means ‘to have an offensive smell’. The spelling ‘foetus’ is therefore not merely incorrect, but might be regarded as being gratu-itously unkind to the healthy fetus (From Reproduction and the Fetus, ALR Findlay, Edward Arnold, 1984.)
During pregnancy, the quality of the environment in the womb is largely determined by the available nutrient and oxygen supply to the growing young. As such, the association between poor conditions in utero and increased risk of heart disease in adulthood has, literally, exploded a new field of research investigating the effects of changes in nutrition during pregnancy on programming cardiovascular disease (McMillen & Robinson, 2005).
However, in contrast to the international research effort, the contribution of reductions in oxygen delivery to the fetus, of the type that can occur during pre-eclampsia or placental insufficiency, to reductions in fetal growth and the developmental programming of cardiovascular disease remains very much under-studied. To address this, the group’s programmes of research has recently adopted a two-prong approach addressing questions in a specific human population and determining mechanisms in specific animal models.
Pregnancy in the Andes
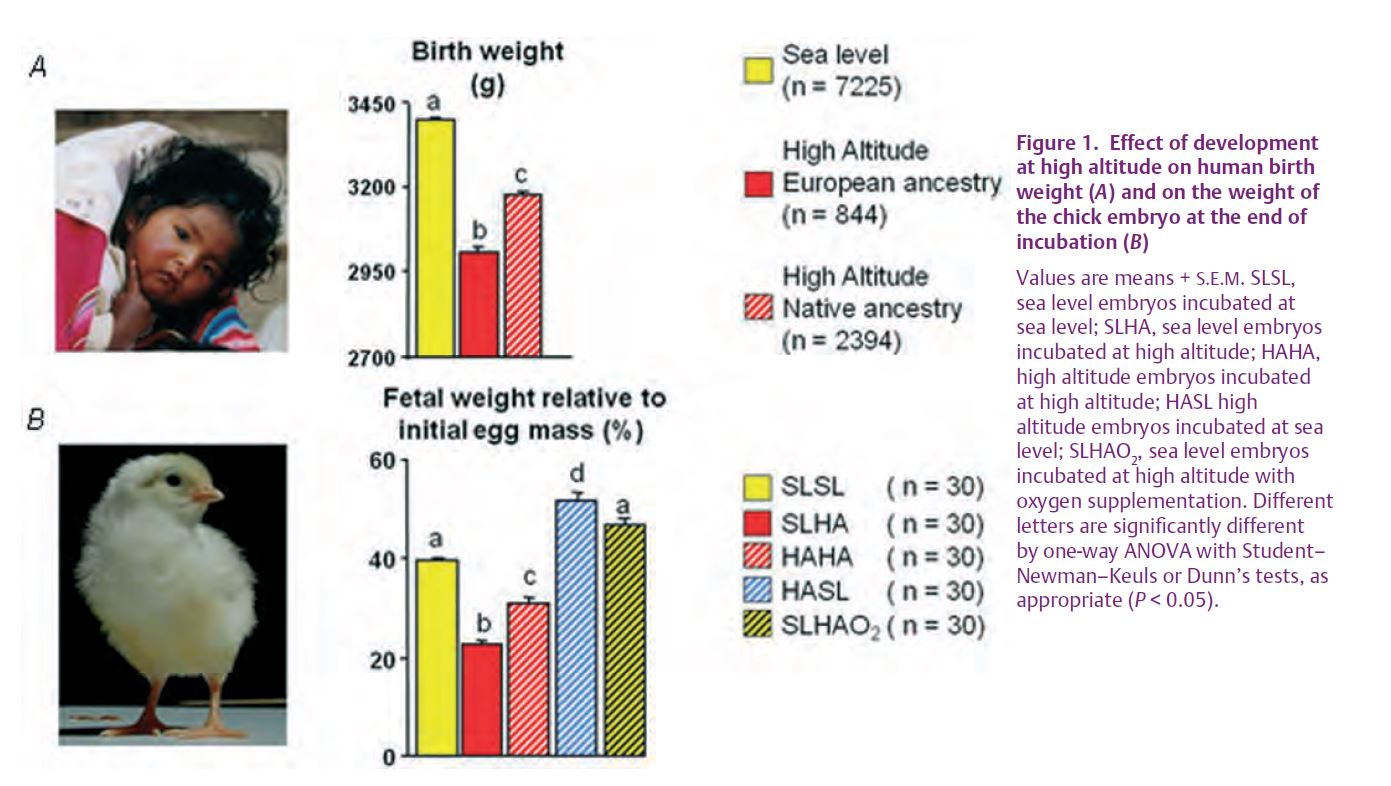
The greater the altitude, the lower the partial pressure of oxygen in the atmosphere. Hence, pregnancy at high altitude is an experiment of nature that permits investigation of the effects of poor oxygenation on fetal development. Epidemiological studies of human populations were carried out in Bolivia (Giussani et al. 2001), as this country is geographi-cally and socio-economically unique. Bolivia lies in the heart of South America and it is split by the Andean cordillera into areas of very high altitude to the west of the country (4000 m) and sea level areas as the east of the country spans into the Brazilian Amazon. Facilitating the study design, the two largest cities, and therefore the most populated with approximately 2 million inhabitants each, are La Paz (4000 m) and Santa Cruz (400 m). Bolivia is also socio-economically unique as both La Paz and Santa Cruz are made up of striking economically-divergent populations. In developing countries, especially in Bolivia, there is an unsurprising strong relationship between socio-economic and nutritional status. Therefore, it was of interest to determine whether the known reduced fetal growth that occurs in the high-altitude regions of Bolivia was primarily due to lack of oxygen in the womb or due to the maternal socio-economic nutritional status. Birth weight records were obtained from healthy term pregnancies in La Paz and Santa Cruz, especially from obstetric hospitals and clinics selectively attended by wealthy or impoverished mothers. Analysis revealed a pronounced reduction in birth weight in babies from high altitude compared with low altitude, despite similarly high maternal economic status (Fig. 1A). Babies born from poor mothers at sea level also showed a reduction in birth weight; however, the effect of poverty was not as pronounced as the effect of high altitude on birth weight. Interestingly, babies born from highland as well as impoverished mothers did not have the greatest reduction in birth weight, as one would have expected. Rather, counter-intuitively, these babies were actually heavier than highland babies born from families with a high socio-economic status! The apparent conundrum was easily explained by assessing the ancestry of the families. The low socio-economic group of La Paz contained a high percentage (92%) of women from Amerindian origin with Aymara indian paternal and maternal surnames. In contrast, the high socio-economic group of La Paz contained a high European admixture. These findings, therefore, revealed not only that fetal oxygenation relative to fetal nutrition was an important deter-minant of fetal growth, but also that prolonged high altitude residence ancestry conferred protection against this effect. Reduced fetal growth at altitude is correlated with the duration of high altitude residence, independent of maternal nutrition: the longest resident population experiencing the least decline and the shortest residence groups demonstrating the most reduction in birth weight (Fig. 1A). Accordingly, reductions in birth weight at elevations greater than 3000 m above sea level are greatest in Colorado, intermediate in Andeans and least in Tibetans (Moore, 1990).


Mountain chicks hatch clue to fetal development
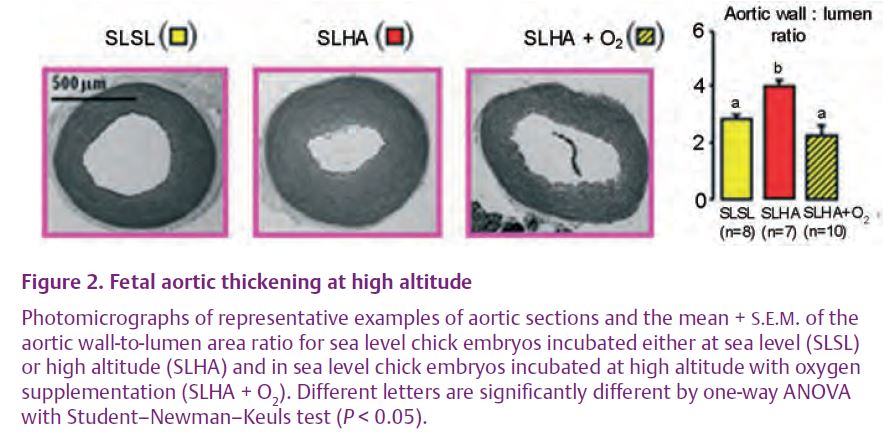
The second prong of our approach exploited the chick embryo as an animal model. In contrast to all mammals (bar monotremes), in avian species the effects on the fetus of lack of oxygen can be studied directly, without additional effects of hypoxia on the mother and the placenta, and without the confounding problems of poverty and ethnicity in highland human populations. A recent study published in The Journal of Physiology (Giussani et al. 2007) reasoned that if oxygen alone had a real role in the direct control of fetal growth and a developmental origin of heart disease, then fertilised eggs from hens native to sea level should show growth restriction and an increased risk of heart disease when incubated at high altitude. In addition, the experiment could be done the other way around, something almost impossible to test in human popula-tions. Hence, fertilised eggs from hens native to high altitude could be incubated at sea level to determine if the fetus recovers its growth and the risk of heart disease is normalised. Again, the study was done in Bolivia. The data show that incubation of sea level embryos at high altitude led to a 50% growth restriction, but incubation at high altitude of embryos from hens native to high altitude only led to 30% growth restriction (Fig. 1B). Furthermore, incubation at sea level of embryos from hens native to high altitude not only restored growth, but these embryos were actually larger than sea level embryos incubated at sea level. Interestingly, incubations at high altitude, irrespective of highland ancestry, led to an increase in the thickness of the walls of the fetal heart and of the fetal aorta – early markers of cardiovascular disease. Reassuringly, these effects of high altitude development on cardiovascular remodelling could be prevented by incubation at sea level or by incubation at altitude with oxygen supplementation (Fig. 2).
Vitamin C and health interests grow: bringing the Andes to Cambridge
The group’s latest programmes of research have established that the adverse effects of prenatal hypoxia on cardiovascular development may be secondary to the generation of oxidative stress. If true, this is an exciting possibility to combat the developmental programming of heart disease as it offers the potential for treatment with antioxi-dants of pregnancies complicated with reduced oxygen delivery to the fetus, be it at sea level, such as during pre-eclampsia or placental insufficiency, or during pregnancy at high altitude. The latest data show that exposure of pregnant rats to reduced oxygenation at normal barometric pressure here in Cambridge does not affect maternal food intake but it yields offspring with cardiovascular problems
both at the end of gestation and in adulthood. Importantly, these effects of hypoxic pregnancy can be prevented by giving the mothers antioxidants in the drinking water. This latest work not only highlights that fetal oxygenation independent of nutritional and genetic risk factors is a potent trigger for a prenatal origin of heart disease, but the antioxidant findings provide science a unique and timely opportunity to bring ‘preventative medicine back into the womb.’
References
Barker DJP (1998). Mothers, babies, and disease in later life. Churchill Livingstone, Edinburgh.
Giussani DA, Phillips PS, Anstee S & Barker DJ (2001). Effects of altitude versus economic status on birth weight and body shape at birth. Pediat Res 49, 490–494.
Giussani DA, Salinas CE, Villena M & Blanco CE (2007). The role of oxygen in prenatal growth: studies in the chick embryo. J Physiol 585, 911–917.
McMillen IC & Robinson JS (2005). Developmental origins of the metabolic syndrome: prediction, plasticity, and programming. Physiol Rev 85, 571–633.
Moore LG (1990). Maternal O2 transport and fetal growth in Colorado, Peru and Tibet high-altitude residents. Am J Hum Biol 2, 627–637.
Group sponsored by The British Heart Foundation, the BBSRC, The Lister Institute for Preventive Medicine, The Royal Society and The Wellcome Trust. Dino Giussani is a member of the Cambridge Centre for Trophoblast Research.
Members of the research group: Dino Giussani, Emily Camm, Hans Richter, Emilio Herrera, Jez Hansell, Andrew Kane, Carlos Salinas, Rudy Soria, Avnesh Thakor, Ali Adler, Carlos Blanco & Youguo Niu.