
Physiology News Magazine
Is daylight worth saving or is it time to change?
The health controversies around daylight saving time
Features
Is daylight worth saving or is it time to change?
The health controversies around daylight saving time
Features


Dr Philip Lewis & Professor Thomas C Erren
Institute and Policlinic for Occupational Medicine, Environmental Medicine and Prevention Research, University Hospital of Cologne, Germany
Daylight saving time (DST) is an advanced official clock time, typically by 1 hour, and typically employed during months with longer durations of daylight (e.g. from the last Sunday in March to the last Sunday in October, in the EU and UK). The desired result is that sunrise and sunset occur at an official clock time that is 1 hour later. DST is then changed back to “standard time” (also known as “winter time”) for months with shorter durations of daylight. This biannual transition is practised in most of Europe and North America and in some parts of South America, Oceania, and Asia. Many countries not currently employing DST have experimented with it in the past. The “spring forward” (DST onset) and “fall back” (DST offset) transitions have caused controversy for many decades and on many levels, including potential complex health and economic effects, and simple inconvenience and practicality. Furthermore, the manner in which changes in official clock times affect the relationship between social schedules, sunshine hours, internal “circadian” time, and health will differ by geographical, cultural, and individual factors. From a health sciences perspective, DST offers an incredible natural experiment opportunity to be explored. As DST debates (including whether to abolish the time change and to keep either standard time or DST) gather momentum, DST-policy changes, at least in some regions, seem inevitable. Therefore, this natural experiment must be appropriately utilised to help reconcile health controversies.
Brief history of (adjusting) time
The adjustment of clock time is nothing new. For instance, water clocks used in ancient Mesopotamia, Egypt, Greece, China, India, and Rome had different scales for different months, making time intervals within a day longer or shorter as necessary in alignment with daylight hours. Sundials could only indicate time when the sun was shining, and daylight hours vary with season. Furthermore, the gnomon of a horizontal sundial must be parallel to the Earth’s axis for accurate time; this was not always the case. Sundials could be used to determine local solar time only, the reference for which is when the sun reaches its highest point (or zenith) in the location of the observer. Thus, towns and villages had their own local time zones. The use of equal hours (i.e. 60 mins in every hour) in a 24-hour day may have become more widespread with the development of spring clocks in the 14th-15th century and with traders needing more accurate, secular time keeping for commercial benefit.
Although equal hours were increasingly used, local solar time remained common (and a person would have to adjust their clock if travelling from e.g. London to Dublin). In 1884, “The International Meridian Conference” facilitated propagation of the time zones concept in scientific-political discourse in many countries. However, it took many decades before a significant number of countries adopted the time zone concept and the Greenwich meridian was taken as the reference point for universal times and time zones (longitude 0o, UTCs).
The first serious proposition of biannual adjustments to standardised clock time came about a decade after the 1884 conference. In 1895, George Hudson put forward the idea of a 2-hour shift in New Zealand so that daylight hours would overlap with his offwork entomology hobbies. The next known suggestion by William Willett in London (1907) involved four shifts by 20 mins each over consecutive Sundays after noticing many people slept after sunrise and yet he had not enough daylight for golf in the evening (Douma, 2008). None of these suggestions were implemented.
The first city to employ DST was Port Arthur in Canada in 1908, while the first states to employ DST were the German and Austro-Hungarian Empires during World War I – to conserve coal. Other countries quickly followed suit. More countries adopted DST during World War II and more again during the energy crisis of the 1970s.
The specific calendar days when transition to and from DST occurred and the size of clock change on transition days has varied by region and year. For instance, a 2-hour shift was employed in the UK during World War II and again in 1947. Currently in the EU and the UK, a 1-hour advance occurs on the last Sunday in March (DST onset) and DST offset occurs on the last Sunday in October. Different DST practices in Europe were considered disruptive to transport and communications, leading to directives from the European Commission for transition day alignment since 1981.
Brazil makes for a good case study in DST practice variability. In Brazil, DST transition dates were set one year at a time until 1968 when onset was fixed as the first day of November and offset as the first day of March, regardless of the day of the week. Note that the month–daylight relationship is inverse for the southern hemisphere, and most Brazilian states are south of the equator, hence, the inverse time-of-year onset and offset compared to the northern hemisphere. In 1987, transition days in Brazil were fixed to Sundays. By 1991, 15 of the 27 Brazilian states, all from the north and northeast regions abandoned DST practices. From 2008, DST onset was fixed as the 3rd Sunday in October and offset as the 3rd Sunday in February unless this coincided with Carnival, with offset then being delayed by one week. As of 2020, no Brazilian states employ DST.
Current debate in Europe and the USA
Following the results of a citizen survey in 2018 (European Commission, 2018) the European Commission proposed to end biannual clock changes. However, no approval by parliament and council has yet been made due to discrepancies between what member states favour, lack of impact assessments made by member states, and the COVID-19 pandemic delaying proceedings. Of note, a slight majority of the 2018 citizen survey were in favour of keeping DST all year round (i.e. perennial DST). However, the representativeness and generalisability of the survey results are highly debatable (Blume and Schabus, 2020).
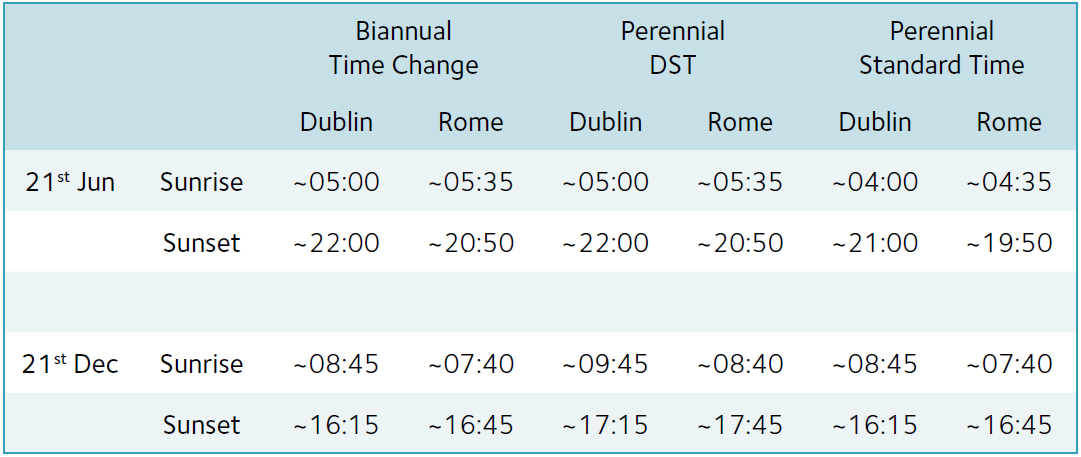
In terms of public perception of DST, Coogan et al. (2022) use the example of Dublin and Rome to highlight potential differences; for instance, abandoning DST for perennial standard time may be more negatively appraised in Rome (with sunset before 8pm in summer) than in Dublin (Table 1) (Coogan et al., 2022).
The UK leaving the EU in 2020 (“Brexit”) throws another spanner in the works for Europe. The UK government has no current plans to abandon DST practice. If the EU abandons DST practice, there would be a 1-hour time difference between Northern Ireland and the Republic of Ireland for approximately half of the year, which is unfavourable to locals (Coogan et al., 2022).
In the USA in 2022, the Sunshine Protection Act (US Senate, 2019) – which involves the implementation of permanent DST – was approved by the Senate but is yet to be approved by the House of Representatives. The name of the proposition – “Sunshine Protection” – is certainly non-neutral in terms of how it may be perceived.
In popular media, and often in scientific circles, the debate is framed as choosing between perennial DST and perennial standard time. Arguments for and against include both health and economics. Consumption of resources, as was central to DST origins due to the World Wars and energy crises, may again be an issue in some places. Reliance on Russian oil and gas in Europe has been highlighted since the condemned Russian invasion of Ukraine. Seemingly lacking from popular debate is whether biannual transitions should be maintained or even modified (such as changing transition dates).
Health controversy
Regarding health, the principal “exposure” talking points are: (1) acute transition to and from DST, (2) the DST period for a given year and across many years (as opposed to standard time during these periods), and
(3) the standard time period for a given year and across many years (as opposed to DST during these periods). The principal “outcomes” studied mainly concern the acute effects of transitions, and include potential brief differences in the incidence of acute myocardial infarction (AMI) (Manfredini et al., 2019), traffic and other accidents (Fitz et al., 2020; Lahti et al., 2011), and all-cause mortality (Levy et al., 2022). The principally discussed “potential physiological drivers” linking exposures to outcomes are changes to sleep and circadian rhythms, and to stress and anxiety in the lead-up to transition days.
Acute transition
To the best of our knowledge, only studies of AMI have been subjected to a meta-analysis, with increased risk of AMI following DST onset but not offset observed (Manfredini et al., 2019). Controversies behind these results include that two of the included studies providing high weight to the meta-analysis involve overlapping populations, that no critical appraisal of the studies involved was provided (including the extent as to whether pooling was justified), and that large differences in risk estimates between some studies suggest that at least some are heavily biased. There is evidence of increased traffic accidents following DST onset in the USA (Fitz et al., 2020), but questions arise regarding how great a role was played by the consequent changes in illumination during major commute times (Martin-Olalla, 2020). DST offset, but not onset, was associated with a spike in all-cause mortality in Europe, which is in contrast to what might be expected given the observations regarding traffic accidents and AMIs with DST onset (Levy et al., 2022). A study from Finland concluded effects of DST transitions were not harmful enough to have an impact on occupational accident rates (Lahti et al., 2011). However, there are mixed findings for many outcomes in the scientific literature. Reaching a consensus on potential DST transition effects on health would appear to require a stronger evidence base. Effect sizes are small and not consistent, but this does not rule out causal effects. Identifying who is at risk of negative health outcomes is difficult when using registry-based information and taking the large and diverse EU or USA as the regions of interest as wholes. Geographical and individual differences may play a role and investigation of these factors may be useful in debate. The plausibility of the hypothesised mechanisms also come with some controversy; the section below deals with the mechanism.
DST in winter or standard time in summer
Consideration of DST in winter or standard time in summer comes with difficulty. Cohorts of individuals with sufficiently similar geography, culture, and sociodemographic characteristics, but who differ only by either DST or standard time are at a premium, and ruling out potential confounders in studies of these populations would be very difficult. The potential health differences are hypothesised based on circadian biology and potential changes in behaviour are discussed below.
Light, time and circadian controversy
Timing of social schedules and 24-hour rhythmic light-dark exposures are important for our circadian biology. In order to discuss potential biological mechanisms driving potential DST-associated health outcomes (mainly circadian biology-related), we must first understand the relationship between official clock time, time zones, local solar time, and individual internal circadian time – the examples below will help.
Official times and sun times
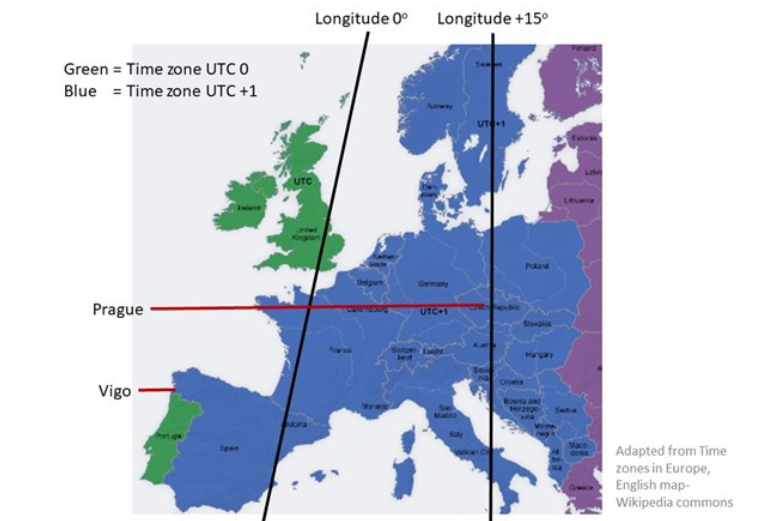
On standard time in Greenwich in the UK (time zone: UTC 0), the sun crosses the Greenwich meridian (or longitude 0°) at noon (or official clock time: 12:00), and is at its zenith in the sky. On DST, the sun reaches its zenith at official clock time 13:00. While the official time of sunrise and sunset will vary in accordance with seasonal trajectory, the official timing of the sun’s zenith will be constant at 12:00 for standard time and 13:00 for DST along the longitude 0° meridian. On standard time, in the UTC +1 time zone (i.e. the clock time is 1-hour advanced compared with UTC 0), the sun reaches its zenith at the longitude +15° meridian (or 15° east) at noon. The +15° meridian approximately follows the German-Polish border and alongside Prague (Prague is located at +14.4°). On DST, the sun will reach its zenith at this meridian. As this meridian is 15o east of the Greenwich meridian, and the time zone is UTC +1, a given solar time (e.g. sun zenith) and corresponding official clock time (e.g. 12:00) at this location will occur one hour before these times occur at the Greenwich meridian.
Along the time zone meridian and during standard time, the solar time reference point – i.e. sun zenith – will be equal to noon. If we move east or west from the meridian but remain in the same UTC time zone, local solar time will occur at an earlier or later official clock time, respectively. In comparison to Prague, the city of Vigo in Gallician-Spain, at longitude -8° (or 8° west) but also in UTC +1, experiences the sun at its zenith at official clock time ~13:40 (1.67 hours after official clock time 12:00 when the zenith occurs at longitude +15°) on standard time and at official clock time ~14:40 on DST. This discrepancy between solar time and official clock time (discrepancy insofar as compared to Prague) occurs because Vigo is some distance west of the +15° meridian for the UTC +1 time zone (Fig .1).
Internal time
The internal circadian timing system (CTS) receives light information from specialised light sensitive cells in the eyes that project to a “master” circadian clock in the suprachiasmatic nuclei of the hypothalamus. The master clock has direct and indirect neuroendocrine projections to the clocks in every other cell in the body (so-called peripheral clocks). Each cellular clock is composed of a genetic-transcriptiontranslation-feedback-loop (the specific genes involved are known as clock genes) lasting approximately 24 hours that give rise to circadian rhythms in cellular physiology. The master clock receives information about the 24-hour light-dark zeitgeber (time cue) rhythm and entrains to it (it can take a few days to entrain to a new zeitgeber rhythm – which can cause the jet lag associated with rapid travel across time zones) (Lewis and Erren, 2021). The master clock will subsequently assist entrainment in the peripheral clocks. When entrained, cellular circadian rhythms will now be in-sync, and the highs and lows in rhythmic functions that are beneficial to our physiology can now occur and at an appropriate time relative to the external time cue. For example, metabolism will start ramping up for activity during the light part of the zeitgeber rhythm and slowing down when it is time to sleep during the dark part of the zeitgeber rhythm. It can be helpful to consider our circadian-entrained sleep time as the biological night and our circadian entrained wakeful time as the biological day. The biological night and biological day make up our internal time.
In our modern society, our light-dark zeitgeber rhythm consists of different intensities of daylight, artificial light, and darkness. The latter is typically our exposure when going to sleep as we seek darkness and then close our eyes. The zeitgeber rhythm phase then typically includes higher light intensities after wakening, during waking hours, and lower intensities as we again approach the biological night. The timing and intensity of light experience is important. In times before artificial light, we would entrain to the natural light-dark cycle that occurs because of the Earth’s 24-hour rotation on its axis. Nowadays, our biological nights and days do not necessarily follow local solar time because of social schedules and artificial light, but we still have a penchant for scheduling social activity to overlap with at least some daylight hours. Daylight intensity is often orders of magnitude higher than artificial light and can provide an important and stronger zeitgeber effect.
Thus, an advance or delay in clock time and consequent advance or delay in social schedules (as school, work, and appointment times are typically at set times) with transitioning between standard time and DST can affect our circadian rhythm because the rhythm phase when light is experienced will change. As the CTS entrains to the new zeitgeber rhythm (i.e. the zeitgeber rhythm phase is 1-hour shifted), there can be periods of internal rhythm misalignment as different internal clocks shift at different speeds, and this may cause damage (Pittendrigh, 1960). The acute CTS shift required for DST onset and offset may be considered minor and somewhat comparable to the shift needed to flying to a new time zone with a 1-hour difference from place of origin (Lewis and Erren, 2021). Of course, some individuals may be more susceptible to the impact of transient misalignment.
Sleep
Regarding sleep, if we do not try to adapt to DST onset in advance, sleep can be cut short by 1-hour for those who must get up at a certain time to fulfil social obligations such as work and school. Again, a 1-hour difference for 1 night only might be considered minor but some individuals may be more susceptible. If a few days are required for entrainment (i.e. setting our internal clocks to the shifted zeitgeber) the sleep-wake cycle may also be transiently perturbed as it is co-controlled by the CTS.
Controversy
Regarding circadian biology controversy, individual susceptibilities may explain acute health effects following transitions, but what about perennial DST or perennial standard time? Even though our light exposure may change by 1 hour at transition, the duration of time between zeniths of the sun does not (i.e. the sun zenith occurs almost precisely 24 hours after its previous zenith, regardless of official clock time change). Advocates against keeping the time change (and against keeping DST if the change is abolished) argue that our social schedules match solar time more accurately when we use standard time and that our internal times would then also (Roenneberg et al., 2019). Now, the importance for the CTS of strong light shortly after awakening is probably the most often cited element of circadian biology for public health. This is certainly the case in mid-latitude winter and is why sleep and circadian researchers are against perennial DST. Sunrise would not occur until after 09:00 in London in mid-winter; the majority of people will waken between 06:00 and 08:00 for school and work. Sunrise may be as late as 10:00 in the city of Vigo in Spain if DST were used in winter. For summer months, DST may be more favourable than standard time and the internal time more closely matching solar time” argument (indeed, whatever “closely matching” actually means) should be less problematic. Mid-summer sunrise in London will be ~04:30 on DST and would be 03:30 on standard time. The majority of people will not require first light exposure before 04:30 so potential morning light unavailability is much less of a problem compared to winter months. For those less well able to find or create darkness for sleep – for instance due to the cost of light-blocking curtains or requirement to keep curtains and windows open to let cooler night air inside in summer – 03:30 sunrise may be more detrimental to their circadian biology. Shift workers travelling home after the late shift are more likely to be exposed to the earlier sunrise before sleep, which may be detrimental to their circadian biology.
Beyond sleep and the circadian timing system
As mentioned already, illumination, or lack thereof, on commutes also presents dangers (Martin-Olalla, 2020). Depending on local sunrise and sunset times, morning or evening commutes may be affected by increased morning or evening daylight. Pro-perennial DST arguments also cite reduced crime with more evening daylight at the expense of less morning daylight, and more time for children to play outside during daylight hours on winter evenings. How these arguments are perceived is also likely to be affected by actual sunset times and outdoor temperature, in addition to individual factors such as sex and age.
Additional pro-DST during summer arguments include that those attending animals, such as farmers and families with pets, may have to arise very early to tend to animals on standard time during the summer and this may hinder social obligations that occur later in the day.
What can we do?
For circadian biology, DST may be more preferable to sunrise and social schedule relationships during summer rather than winter for the reasons outlined above, and is contrary to the position of many sleep and circadian biology societies. Findings of acute health effects of transition are controversial and mixed findings need to be reconciled. Changing transition dates to prevent sudden and dramatic changes in illumination levels during commute rush times in some regions should be considered. In addition to reconciliation of
controversies, trade-offs between potentially beneficial DST in summer and potentially detrimental health effects of transition to and from DST need to be weighed against each other. Use of resources and economics also need to be considered alongside health in terms of how DST or standard time may affect the consumption of resources. Local geography (in particular latitude and longitude), time zone, and culture (e.g. early and late risers) are also important aspects to be considered.
For the individual, step-by-step or gradual adaptation in advance of transition days, especially by those more susceptible to an acute health event, should help to reduce potential risks. In line with Willett’s 1907 idea of gradual adaptation, four days of shifting sleep and wake times by 15 mins might be helpful (Douma, 2008). In some cases, it may simply help to reschedule the clock time of a social obligation to better suit local solar time. This may be facilitated nowadays following the increased use of home offices after the COVID-19 pandemic. Ultimately, the latter requires appropriate dissemination of advice from Public Health and requires agency on the part of individuals.
All-in-all, the jury is still out regarding the best policy decisions to make and this is before looking beyond circadian biology. Dropping the biannual time change may be neither beneficial nor necessary, but this is a controversial standpoint.
References
Blume C and Schabus M (2020). Perspective: daylight saving time-an advocacy for a balanced view and against fanning fear. Clocks & Sleep 2, 19-25. https://doi.org/10.3390/clockssleep2010003
Coogan AN et al (2022). A data-informed perspective on public preferences for retaining or abolishing biannual clock changes. Journal of Biological Rhythms 37, 351-357. https://doi.org/10.1177/07487304221096390
Douma M (2008). Daylight saving time – William Willett’s pamphlet (Sloane Sq, London, 1907). https://www.webexhibits.org/daylightsaving/willett.html.
Fritz J et al. (2020). A chronobiological evaluation of the acute effects of daylight saving time on traffic accident risk. Current Biology 30, 729-735 e722. https://doi.org/10.1016/j.cub.2019.12.045
European Comission (2018). Summertime consultation: 84% want Europe to stop changing the clock. https://eur-lex.europa.eu/legal-content/EN/ALL/?uri=CELEX%3A52018SC0406
US Senate (2019). Sunshine Protection Act of 2019.doi:https://www.congress.gov/bill/116th-congress/senate-bill/670/text.
Manfredini R et al. (2019). Daylight saving time and acute myocardial infarction: a meta-analysis. Journal of Clinical Medicine 8. https://doi.org/10.3390/jcm8030404
Lahti T et al. (2011). Work-related accidents and daylight saving time in Finland. Occupational Medicine (Lond) 61, 26-28. https://doi.org/10.1093/occmed/kqq167
Levy L et al. (2022). Daylight saving time affects European mortality patterns. Nat Commun 13, 6906. https://doi.org/10.1038/s41467-022-34704-9
Lewis P and Erren TC (2021) Avoiding the traveller’s blues. Physiology News 122, 22-25. https://doi.org/10.36866/122.22.
Martin-Olalla JM (2020). Traffic accident increase attributed to Daylight Saving Time doubled after Energy Policy Act. Current Biology 30, R298-R300. https://doi.org/10.1016/j.cub.2020.03.007
Pittendrigh CS (1960). Circadian rhythms and the circadian organization of living systems. Cold Spring Harbor symposia on quantitative biology 25, 159-184. https://doi.org/10.1101/sqb.1960.025.01.015
Roenneberg T et al. (2019). Daylight saving time and artificial time zones – a battle between biological and social times. Frontiers in Physiology 10, 944. https://doi.org/10.3389/fphys.2019.00944