
Physiology News Magazine

Physiology in the extreme: The case for microgravity research
Why should UK life scientists be excluded from the opportunity of using space agencies’ resources to study problems of major physiological and clinical interest?
Features
Physiology in the extreme: The case for microgravity research
Why should UK life scientists be excluded from the opportunity of using space agencies’ resources to study problems of major physiological and clinical interest?
Features
Marco Narici (1) & Michael Rennie (2)
1: Institute for Biophysical and Clinical Research into Human Movement, Manchester Metropolitan University, Alsager, UK
2: Graduate Entry Medical School, University of Nottingham, City Hospital Derby, UK


https://doi.org/10.36866/pn.61.19
A few days ago (19 September), NASA’s administrator Dr Michael Griffith announced detailed plans for returning to the Moon by 2020. The intention is to establish a permanently manned lunar station, with crew shift durations of up to 6 months, and eventually, to extend human presence in the solar system and beyond.
However, before these long-term goals can be achieved, there are a number of obstacles that need to be overcome. Exposure to microgravity notoriously affects the major physiological systems, amongst which the musculoskeletal, cardiovascular, nervous, hormonal and immune systems are the most affected. Pertinantly, whereas changes to the cardiovascular, nervous, hormonal and immune system are reversible within a relatively short time upon return to life at 1 g, and some may be mitigated by in-flight exercise countermeasures (e.g. the cardiovascular, the respiratory and motor control changes), those affecting the musculoskeletal system are more difficult to protect and to reverse. It has been estimated that the loss of muscle and bone may be as much as 1-2% per month under weightless conditions, a rate which would render a 36 month trip to Mars and back extremely hazardous for the participants, who would suffer a grave risk of their remaining lives as cripples on Earth. However, muscle atrophy and osteopenia are not only a problem upon return to 1 g, but also during spaceflight since preservation of mobility is vital for tasks such as extra vehicular activities (EVAs) and during surface activities, dealing with emergencies. Another major problem is that of shielding astronauts from solar radiation, but although this is likely to be difficult, it should not be insuperable.
Nevertheless, one fundamental issue is that the long-term effects of exposure to spaceflight conditions are actually unknown. For example, the bone loss is apparently reversible after 1-2 years but the changes in bone microstructure do not seem to be fully reversible. Another isssue of great concern is the effect of trace gases and changes in microflora on an already weakened immune system, which may lead to an increased cancer risk in the long term.
The major space agencies (National Aeronautics and Space Administration (NASA), European Space Agency (ESA), Japanese Space Agency (JAXA), Russian Space Agency (Roskosmos) and now even China) invest vast funds each year in support of research programmes aimed at the study and prevention of the physiological deconditioning induced by actual and simulated microgravity. As far as ground-based studies are concerned, Europe can claim some of the best facilities for short and longterm bed rest experiments, the French Institute for Space Medicine and Physiology (MEDES) (www.medes.fr) and the German Aerospace Centre (DLR) (www.dlr.de/me). For 2002-2006 alone, ESA has committed about €90M to human spaceflight and microgravity research: it is just about to launch a new 3 year campaign of short (5 day) and long-term (60 day) bed rest studies. These initiatives are of great scientific interest since they provide the opportunity to perform many investigations on healthy individuals undergoing bed rest under highly controlled conditions and with access to excellent wide range facilities such as magnetic resonance imaging (MRI), dual-energy X-ray absorptiometry (DEXA), micro-computed tomography, human centrifuges, climate chambers, rotating chairs, lower body negative pressure, high resolution echography and tissue engineering, to mention a few.

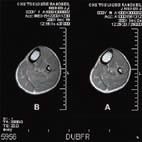
For instance, in one of the recent bed rest studies organised by ESA at the MEDES clinic in Toulouse (http://www.medes.fr/Clinic/Experiments/LTBR/), we were able to demonstrate that about 30% of calf muscle mass is lost after 90 days of inactivity (Fig. 1), even though individuals performed regular, highintensity, exercise countermeasures effective in preventing atrophy of the thigh muscles (Reeves et al. 2005; Alkner and Tesch, 2004). From a clinical point of view, such loss of muscle mass is particularly concerning since a loss of muscle mass greater than 40% is normally considered a serious health-hazard (Morley et al. 2001). As a matter of fact, over four and a half months on the Mir Space Station astronaut ‘A’ lost 40% of his body’s muscle mass, 12% of his bone mass, and 23 pounds. After astronaut ‘A’ returned to Earth it took six months to recover the lost strength, and a year to recover the lost bone mass. Two other astronauts who stayed over four months still have bone deficits after more than 2 years on Earth (see NASA archives: http://members.nova.org/~sol/station/hazards.htm) Thus, it appears that unless some means is found to create artificial gravity in space, for example by building a vehicle which spins around its axis with living quarters at the periphery or an exercise device which itself produces gravity (di Prampero & Antonutto, 1997; di Prampero, 2000) or the use of a human centrifuge (that ESA will have available for the scientific community early next year) then counter measures will have to be developed to prevent muscle and bone wasting.
Why microgravity simulation on earth is not enough
Research on the problem has adequately defined its extent by studies of astronauts during and after spaceflight and there have been three rather clear lessons. First, the rate of loss of muscle and bone are much greater than observed during model situations on Earth (such as head down bed rest); secondly, wasting, at least of bone, continues for some time after the return to full gravity on Earth (Rittweger et al. 2005) so that rehabilitation may take months to years; and thirdly, that all the counter measures which have been hitherto applied, (including a variety of Heath-Robinson contraptions involving straps, elastic cords, treadmills, bicycles, etc) have only partly mitigated, but not prevented, the losses. It appears reasonably obvious that simple muscular contractions, even those contractions which impose some force on bones and tendons, do not sufficiently to mimic the effects of loading in gravity (Alkner & Tesch, 2004; Reeves et al. 2005)
Perhaps this is one of the reasons why studies of bed rest have yielded results sometimes in contrast with those obtained in actual microgravity. In simulated microgravity, such as bed rest, individuals are studied under highly controlled conditions and their activity levels can be closely monitored. In microgravity, accurate levels of physical activity are often not recorded or reported and physical countermeasures are prescribed by the crew surgeon with no control of the investigators (Kozlovskaya and Grigoriev, 2004). Furthermore, unlike simulated microgravity, exposure to true zero-g has been shown to directly induce a reduction in myofibrillar and connective tissue protein synthesis (Vandenburgh et al. 1999). This strongly suggests that there is something about gravity which has an effect even in the 6 ° head-down tilted position which tends to maintain musculoskeletal mass and which is missing in space. However, head-down bed rest remains the model of choice for simulating the effects of microgravity on earth.
What could we do with access to astronauts making short space visits?
If we hypothesize that there is such an entity within muscle and bone as a ‘gravity sensor’ then it seems plausible to suppose that this sensor is a protein which is coded for by messenger RNA produced after transcription of genes in the nucleus. The best way to identify the sensor would be by searching for gene expressions which are present in circumstances of full gravity and missing in circumstances of zero gravity when there would be an infinite step change between the two conditions. Our current evidence suggests that the anabolic influence of the gravity sensor remains reasonably strong even under conditions of bed rest and therefore in order to detect changes in gene expression we need a rapid square wave diminution/ restoration of the force of gravity with samples taken before and after. This is exactly what could be done in studies of astronauts on the International Space Station (if Britain were signed up to the programme!).
It is perfectly feasible with current technology to compare samples of muscle and bone taken from astronauts before going into space, immediately after a sojourn of say a week (which is likely to be long enough to cause the changes in gene expression) and then on their return from space and at intervals thereafter. Muscle and bone biopsies are much less invasive than generally supposed and are painless with appropriate local anaesthetic; they are without long term consequences if carried out using appropriate techniques. By comparing the expression of genes under normal gravity conditions and immediately after returning from zero gravity it ought to be possible to identify those genes likely to be involved in the sensing of gravity and the signalling of the sensory correlate to processes ultimately as controlling muscle and bone masses.
The technology is certainly available now with incredibly powerful DNA and proteomic array “labs-on-a-chip” (e.g. Albala, 2001; Chittur, 2004), and there are several precedents for gene expression experiments conducted on human space missions (e.g. Taylor et al. 2002; Wilson et al. 2002; Semov et al. 2002). Having identified the sensor, it ought to be possible to design ways of intervening in its actions by pharmacologically blocking or enhancing parts of the signalling pathway in order to ameliorate the effects of loss of gravitational influences on anabolic and catabolic processes in muscle and bone.
The possible benefits
Of course this does sound like science fiction – but all future scientific projections are science fiction until they become a reality. We certainly have the technical capabilities to identify the gravity sensor in the way we have described above and there are major pressures which would help encourage the pharmaceutical industry to become involved in solving the problems of which genes are transcribed their protein products and how it would enhance or diminish their influence by pharmacological means.
What do we mean by major pressures? Currently in the developed countries the increase in life expectancy which has come as a result of effective conquering of most infectious diseases and better nutrition, has caused a rapid growth in that segment of the population which is over 60. We know that muscle and bone loss occurs in this group at a rate of about 15-20% per decade beyond the age of 50 and that these musculoskeletal losses have major implications for the individual and society in terms of loss of dependence and therefore an increase in dependence upon family, neighbours and the state, but also in terms of increased medical costs due to falls and fractures. Currently there are few strategies which can be successfully applied to the problem. Presently, no effective drugs have been found yet which may fully prevent muscle loss, at best they can only mitigate but not prevent muscle atrophy and the drugs which are used to counter bone loss are sufficiently expensive than we could probably not afford to use them if all of the members of our society who were losing bone were diagnosed adequately. In any case, these drugs are relatively ineffective particularly in terms of the maintenance of bone qualities other than bone mineral density (i.e. content of calcium salts).
If we were able to identify the gravity sensor responsible for the maintenance of muscle and bone and identify ways of enhancing the action of the anabolic signalling pathways, which rationally must be associated with its action, then we could slow or prevent the massive loss of muscle and bone and the huge costs associated with this. In the United States alone the excess costs of sarcopenia alone have been calculated at about $1000 per individual per year and a similar figure is likely to be applicable within Europe. The costs of bone wasting are probably of the same order.
Thus it seems to us that studying human physiology and pathophysiology in astronauts would not only give us the chance of overcoming a major obstacle to manned space flight but would have huge potential benefits here on earth in terms of attempting to deal with the currently intractable medical and social problem of ageing of the musculoskeletal system. Although in this article we have mainly dealt with muscle and bone, similar arguments may be put forward for the other major physiological systems known to be affected by microgravity.
There are, of course, other benefits. One which we believe has been severely underplayed is the very likely halo effect for science and technology education of the human space flight programme. The topic is one which excites the interest and enthusiasm of school pupils and students something which is likely to help reverse the flight from science which we currently experience among young people.
These and other benefits for biological and biomedical and clinical science were recognised by the eminent members of the Microgravity Review Panel (Bill Wakeham, Richard Sykes, Peter Williams and Steve Garwood) set up by Lord Sainsbury, the UK’s science minister, to make recommendations on Britain’s possible involvement in microgravity research. Despite the positive recommendations for this part of the program (Wakeham et al. 2003), no positive increase in the biological aspects of space research has occurred. The UK government has effectively ignored the advice of its experts.
What about the costs?
Even though the costs of maintaining the International Space Station are considerable, the costs of carrying out the clinical research we have discussed above are marginal (e.g. the cost of the current Women International Space Simulation for Exploration (WISE) bed rest study on women totals €3.6M for all agencies) compared to the potential benefits in countering sarcopenia and osteopenia (billions of pounds), and in reversing the internal brain drain away from science. It would be a great pity if we could not grasp the present opportunity to realise these benefits for an expenditure which would be a tiny fraction of the potential return. Unfortunately in the UK we are excluded because Britain does not pay the entrance price of a fill ESA subscription and puts all its eggs into robot missions like the ill fated Beagle project. It has even proved impossible to persuade the Research Councils to ask for special collaborative status for British scientists with NASA and ESA.
Acknowledgements
We are grateful to Drs Didier Schmitt and Patrik Sunblad of ESA for their kind advice and support to this initiative.
References
Albala JS (2001). Array-based proteomics: the latest chip challenge. Expert Rev Mol Diagn 1, 145-152.
Alkner BA & Tesch PA (2004). Knee extensor and plantar flexor muscle size and function following 90 days of bed rest with or without resistance exercise. Eur J Appl Physiol 93, 294–305.
Chittur SV (2004). DNA microarrays: tools for the 21st century. Comb Chem High Throughput Screen 7, 531-537.
Kozlovskaya IB & Grigoriev AI (2004). Russian system of countermeasures on board the international space station: the first results. Acta Astronaut 55, 233–237.
di Prampero PE & Antonutto G (1997). Cycling in space to simulate gravity. Int J Sports Med 18, S324-S326.
di Prampero PE (2000). Cycling on earth, in space, on the moon. Eur J Appl Physiol 82, 345-360.
Morley JE, Baumgartner RN, Roubenoff R, Mayer J & Nair KS (2001). Sarcopenia. J Lab Clin.Med 137 231-243.
Reeves ND, Maganaris CN, Ferretti G & Narici M (2005). Influence of 90-day simulated microgravity on human tendon mechanical properties and the effect of resistive countermeasures. J Appl Physiol 98, 2278 – 2286.
Rittweger J, Frost HM, Schiessl H, Oshima H, Alkner B, Tesch P & Felsenberg D (2005). Muscle atrophy and bone loss after 90 days’ bed rest and the effects of flywheel resistive exercise and pamidronate: results from the LTBR study. Bone 36, 1019–1029.
Semov S, Semova N, Lacelle C, Marcotte R, Petroulakis E, Proestou G & Wang E (2002). Alterations in TNF- and IL-related gene expression in space-flown WI38 human fibroblasts. FASEB J 16, 899-901.
Taylor WE, Bhasin S, Lalani R, Datta A & Gonzalez-Cadavid NF (2002). Alteration of gene expression profiles in skeletal muscle of rats exposed to microgravity during a spaceflight. J Gravit Physiol 9, 61-70.
Vandenburgh H, Chromiak J, Shansky J, Del TM & Lemaire J (1999). Space travel directly induces skeletal muscle atrophy. FASEB J 13, 1031-1038.
Wakeham B, Sykes R, Williams P, Garwood S (2003). Recommendations of the Microgravity Review Panel,
http://www.microgravity.org.uk/recommendations.pdf (also available at http://www.star.ucl.ac.uk/~iac/Microgravity_Report.pdf).
Wilson JW, Ramamurthy R, Porwollik S, McCelland M, Hammond T, Allen P, Ott CM, Pierson DL & Nickerson CA (2002). Microarray analysis identifies Salmonella genes belonging to the low-shear modelled microgravity regulon. Proc Nat Acad Sci USA 99, 1380713812.