
Physiology News Magazine
The role of exercise physiology in 2021
Applying seminal concepts to contemporary issues
Features
The role of exercise physiology in 2021
Applying seminal concepts to contemporary issues
Features
https://doi.org/10.36866/pn.124.28
Dr Paul Ansdell, Northumbria University, UK, Early Career Theme Lead – Human, Environmental, and Exercise Physiology
The past 18 months have been unique for a multitude of reasons, and as I prepared for my PhD viva voce in Spring 2020 I found myself studying cardiopulmonary physiology during the COVID-19 pandemic. As an exercise physiologist by training, I began to consider how the stress imposed by exercise could provide information about this disease’s acute mechanisms; which systems are involved/limited? How do they recover? We now know that long COVID, the persistent symptoms following acute infection, is an issue. So now questions exist such as what underpins these prolonged symptoms? If we know the mechanisms, can we improve recovery? Can exercise testing help answer these questions?
Fast forward 18 months to the Tokyo Olympic and Paralympic Games, and I watched the athletes compete, admiring the pinnacle of endurance physiology during events from 400 metres to the marathon and triathlon. I watched these athletes work to exhaustion, stressing physiological systems that they had strategically trained for the entirety of the previous Olympic cycle and beyond, in awe. Whilst the limiting factors to endurance performance are debated within the exercise science community, one key factor is thought to be the maximal rate of oxidative phosphorylation, the re-synthesis of ATP with oxygen. Here, with elite athletes, performance is the other end of the spectrum to COVID-19 patients; however, the principles of exercise limitation and the methods used to assess them are, broadly speaking, the same. The Human, Environmental and Exercise Theme at The Physiological Society spans a broad range of topics within The Physiological Society, and in this Theme Lead Article, I aim to demonstrate its importance across the spectrum of health and disease, by highlighting recent research in the theme.
The role of oxygen in health and disease
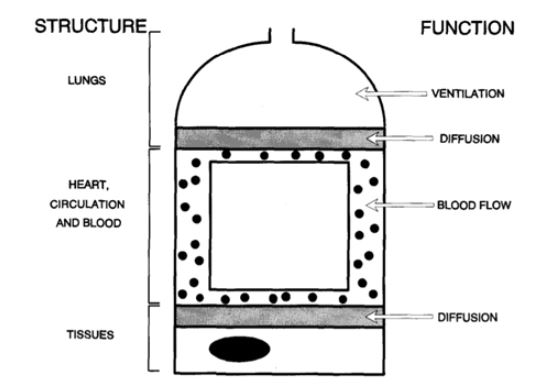
A major part of my viva preparation involved revising oxygen transport and utilisation during exercise in the form of a paper by Professor Peter Wagner: “Determinants of Maximal Oxygen Transport and Utilisation” (Wagner, 1996). This paper reviews the journey of oxygen from the airways to the mitochondria and discusses how changes in this cascade can influence the maximal oxygen uptake (V̇O₂mₐₓ) during exercise. Wagner categorised the oxygen cascade into convective factors, such as ventilation, cardiac output, and red blood cell flow, that permit oxygen transport to the working musculature; and diffusive factors that depend on factors such as capillarity and mitochondria density, which mediate the journey of oxygen across membranes in the lungs and skeletal muscle. He argued that there was no single limiting factor to V̇O₂mₐₓ, that convective and diffusive factors work as part of an integrated system, and that any one component has the potential to alter V̇O₂mₐₓ(Wagner, 2000). Fig.1 demonstrates the structures involved in this system and their individual functions.
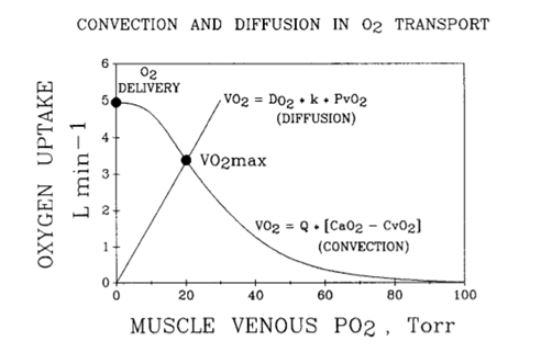
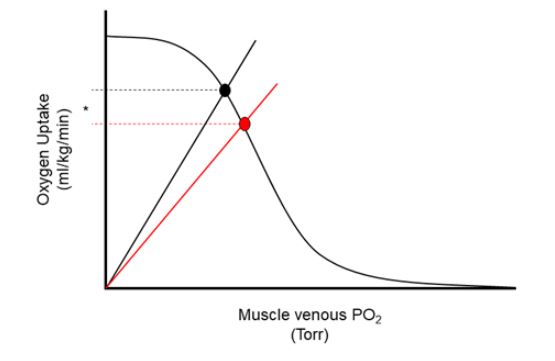
Wagner (1996) also introduced a visual con- struct of this integrated system showing how both convective and diffusive processes can be modelled to predict V̇O₂mₐₓ. Fig.2 demonstrates this, whereby the straight line beginning at the origin represents the diffusive capacity of muscle, underpinned by Fick’s law of diffusion, and the curved negatively sloped line represents oxygen transport through the microcirculation, underpinned by the Fick principle of mass conservation and physiological variables such as blood flow, arterial oxygen saturation, and haemoglobin mass. The point on the y-axis where these two lines intersect determines an individual’s maximum oxygen uptake. As can be seen, the intersect depends on oxygen delivery (cardiac output × arterial oxygen content) and diffusion of oxygen. In turn, arterial oxygen content depends on haemoglobin and arterial O₂ saturation. Arterial O₂ saturation reflects pulmonary gas ex- change. Thus, the intersection point depends on lung function, cardiovascular function, the blood, and muscle diffusional transport in an integrated manner.
This conceptual model is universal in humans and has been used previously to describe how clinical conditions such as chronic obstructive pulmonary disease (COPD) impairs functional capacity, or how increasing altitude can reduce exercise capacity. In the following sections, I will highlight recent physiological research in the theme of Human, Environmental and Exercise Physiology on contemporary issues and topics, such as the Tokyo 2020 Olympic marathon and long COVID, relating back to the Wagner model to provide a conceptual physiological explanation of the findings.
Marathon running and the Tokyo Olympics
Through exercise training, one might improve the ability of the central systems to transport oxygen to the muscle (e.g. cardiac output), raising the curved line. Similarly, exercise training might improve an individual’s capillary density within skeletal muscle, permitting an in- creased diffusive capacity, and increasing the slope of the straight line. In both circumstances, the net result is an increased Y value for the intersection of the two lines: an increased V̇O₂mₐₓ. As one would expect, elite marathon runners demonstrate the optimal physiology, and integrated oxygen transport system, for endurance exercise. Whereby both oxygen transport and utilisation are far superior to the average healthy human, permitting a greater V̇O₂mₐₓ. Indeed, a recent study by Jones et al., (2021) investigated the physiological profiles of the 16 world-class athletes involved in the Nike “Breaking 2” project, which eventually led to the performance of a marathon in 1 hour 59 minutes and 40 seconds by Eliud Kipchoge. Jones et al., demonstrated a mean V̇O₂ peak of 71.0 ± 5.7 mL/kg/min, amongst some other impressive physiological variables, reinforcing the notion that the physiology of elite marathoners is very well suited to running 26.2 miles as fast as humanly possible. Fortunately for spectators, marathon running is deter- mined by more than V̇O₂mₐₓ, however. The pa- per by Jones et al., helps to highlight the physiology required for such a remarkable feat.
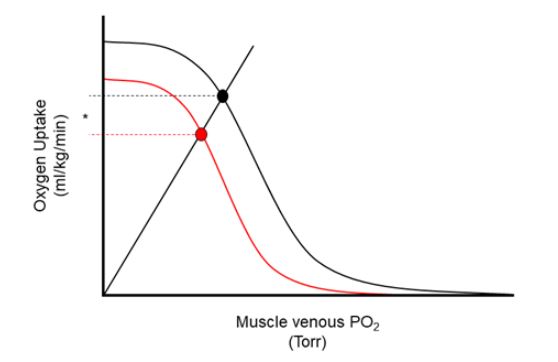
The Women’s Olympic marathon in 2021 took place on 7 August, starting at 6 a.m. local time, and while not unique to Sapporo, the environ- mental conditions during the race were not favourable for optimal performance. At the start of the race the temperature was 25°C and 82% relative humidity, with temperatures peaking at nearly 30°C by the end of the race. The acute effects of exercising in “humid heat” are well studied and relate to the negative consequences of dehydration and hyperthermia. Under such conditions, the physiological determinants of exercise performance can be affected. For example, V̇O₂mₐₓis reduced by up to ~18% in extreme temperatures (Arngímsson et al., 2004). This decline is primarily underpinned by a decrease in cardiac output due to decreased blood volume and the con- sequential negative effects on stroke volume. Additionally, the competition for blood flow between the skin for cooling and the exercising musculature further diverts oxygen from the working muscles in a hot, humid environment. When this is considered in the framework of the Wagner model, a decrease in cardiac out- put would manifest as a downward and left- ward shift in the curved line that represent convection of oxygen to the working muscle. This therefore reduces the y-axis value of where the two lines intersect, and for the exercising athlete, a reduction in V̇O₂mₐₓ(Fig.3). While reduced muscle blood flow has negative consequences for O₂ delivery, it increases red blood cell time in transit through the muscle microcirculation. This provides more opportunity for extraction of oxygen into muscles, a slight buffer to the reduced delivery of oxy- gen, that could otherwise cause even more severe impairments. These alterations in the oxygen transport system mean it is perhaps no coincidence that the winner of the Women’s Tokyo Olympic marathon finished in a time of 2 hours 27 minutes and 20 seconds – nearly 10% slower than the current world record of 2 hours 14 minutes and 4 seconds.
Long COVID
The estimates of long COVID prevalence vary, with the most recent UK Office for National Statistics report stating that 1.9% of the total population (1,200,000 individuals) are currently experiencing prolonged symptoms in the 4 weeks following acute infection (ONS, 2021). The most reported symptoms in the ONS report were fatigue (55%), shortness of breath (39%), and difficulty concentrating (30%); indeed, 65% of individuals reported that their activities of daily living had been adversely affected. Long COVID is therefore a novel problem, that requires the attention of the physiological com- munity in tandem with clinical sciences.
A recent series of studies have highlighted the role that exercise physiology can play in determining the causes of prolonged symptoms, investigating the responses to cardiopulmonary exercise testing (CPET) in long COVID patients. Firstly, Baratto et al., (2021) demonstrated that at discharge from hospital, COVID-19 patients’ V̇O₂mₐₓ was reduced by ~30% compared with age-, sex-, and BMI-matched healthy controls. Although a moderate reduction in respiratory function, assessed via forced vital capacity (the total amount of air that can be expelled from the lungs), was observed, the authors suggested that the primary cause of V̇O₂mₐₓimpairment was due to reduced arterio-venous oxygen difference. This variable represents the ability of working muscles to extract oxygen from the blood.
Following this, Rinaldo et al., (2021) investigated 75 COVID-19 patients with a range of disease severity three months following hospital discharge. The authors split the sample into those demonstrating impaired exercise capacity (V̇O₂mₐₓ< 85% predicted) and those with pre- served exercise capacity (V̇O₂mₐₓ> 85% predicted). In both groups, aspects of respiratory function (forced vital capacity and forced expiratory volume in 1 second) were normal, as were indices of ventilatory efficiency and gas exchange, implying that the pathophysiology associated with exercise impairment was not pulmonary in origin. The primary difference between the two groups was the ventilatory threshold (48 ± 9% V̇O₂mₐₓvs. 62 ± 13% V̇O₂mₐₓ), the point during an incremental test where non-oxidative energy systems begin to contribute more substantially to the resynthesis of ATP. The authors attributed this to an impairment in oxygen extraction with- in skeletal muscle, either directly caused by viral load or the associated muscle deconditioning.
Finally, Singh et al., (2021) studied COVID-19 patients 11 months after acute infection, and importantly, only one of the 10 patients had been admitted to hospital. These patients were compared with age and sex-matched controls, and once again demonstrated no impairment in the function of central physiological systems, when cardiac and respiratory function was assessed. Consistent with the studies of Baratto et al., (2021) and Rinaldo et al., (2021), the patient group demonstrated an impairment in V̇O₂mₐₓ(70 ± 11% predicted). In this cohort, cardiac function and delivery of oxygen was pre- served, whereas peak oxygen extraction in the COVID group was only 62% of that in the control group. The authors argued that the impairments caused by long COVID should not simply be attributed to deconditioning, as function of central physiological systems (e.g. cardiac output, a hallmark of conditioning status) was preserved.
The consistent message between the three studies is that COVID-19 likely induces dysfunction within the microcirculation involved with the diffusion of oxygen, and/or the mitochondria within skeletal muscle itself. Collectively this dysfunction manifests as an impaired ability to extract oxygen from the blood – a key component in the determination of V̇O₂mₐₓ. When considered under the framework of the Wagner model, this would appear as a reduced slope in the straight line representing diffusive capacity, consequently reducing the y-axis value for the intersection of the two lines, implying a reduction in V̇O₂mₐₓ(Fig.4). Given the importance of cardiovascular fitness in predicting functional capacity, quality of life, and mortality in clinical populations, interventions addressing these impairments in long COVID patients must be at the forefront of physiological and medical research.
An example of using the integrated oxygen transport system approach can be found in recent research that demonstrated the mechanisms that underpin adaptation to single-limb exercise training in COPD patients (Broxterman et al., 2021). Specifically, Broxterman et al., showed that muscle diffusive capacity (as measured by the arteriovenous oxygen difference) improved by ~38%. In contrast, convective capacity (as measured by thermodilution-assessed leg blood flow) did not change in COPD patients, constraining overall adaptation. This approach helped the authors to understand the specific pathophysiology associated with the disease, rather than simply attributing impairments to deconditioning.
The role of exercise physiology in understanding contemporary issues
The aim of this article was to use the Wagner model of V̇O₂mₐₓdetermination to contextualise recent events and issues within the theme of Human, Environmental and Exercise Physiology. The integrative oxygen transport system that Wagner describes is universal in mammalian physiology, and by using the frame- work from his seminal 1996 review paper, we can begin to understand how changes to aspects of the system can affect key factors (e.g. V̇O₂mₐₓ) across the spectrum of health and disease. Using the world-class marathon runners profiled by Jones et al., (2021), we can see how years of strategic training optimises an athlete’s physiology for transporting oxygen from the air to the mitochondria to fuel a feat that only one human being has managed to ever perform: a sub 2-hour marathon. The Tokyo Olympics gave us an example of how environmental factors can influence delivery of oxygen to the exercising muscle, worsening performance. Then finally, the recent studies highlighting impairments in the skeletal muscles of long COVID patients demonstrate how we can quantify the integrated oxygen trans- port system, identify mechanisms that could underpin clinical conditions, and begin to work out the best way of treating this growing patient population. Investigating the integrative oxygen transport system in different contexts allows us to quantify and separate convective and diffusive factors, study their interactions, and potentially identify therapeutic targets that might otherwise have been missed. As the early-career theme lead for Human, Environmental, and Exercise Physiology, my goal is to promote our discipline, highlight the work being done, and demonstrate how our theme can integrate with others to advance our understanding of how the human body responds to all types of stressors. The other Theme Leads and I aim to promote Hu- man, Environmental and Exercise Physiology through conferences, workshops, and other initiatives within The Physiological Society. For more information please visit our Theme Page (physoc.org/themes) or see upcoming events (physoc.org/events).
References
Arngrímsson SÁ et al., (2004). Hyperthermia and maximal oxygen uptake in men and women. European Journal of Applied Physiology, 92(4), 524-532. http://doi.org/10.1007/s00421-004-1053-1
Broxterman R et al., (2021). Exercise training in chronic obstructive pulmonary disease: muscle o2 transport plasticity. European Respiratory Journal. In Press. http://doi.org/10.1183/13993003.04146-2020
Baratto C et al., (2021). Impact of COVID-19 on exercise pathophysiology: a combined cardiopulmonary and echocardiographic exercise study. Journal of Applied Physiology 130(5), 1470-1478. http://doi.org/10.1152/japplphysiol.00710.2020
Jones AM et al., (2021). Physiological demands of running at 2-hour marathon race pace. Journal of Applied Physiology, 130(2), 369-379. http://doi.org/10.1152/japplphysiol.00647.2020
Office for National Statistics (2021). Prevalence of ongoing symptoms following coronavirus (COVID-19) infection in the UK: 4 November 2021. https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/prevalenceofongoingsymptomsfollowingcoronavirus-covid19infectionintheuk/4november2021
Rinaldo RF et al., (2021). Deconditioning as main mechanism of impaired exercise response in COVID-19 survivors. European Respiratory Journal. In Press. http://doi.org/10.1183/13993003.00870-2021
Singh I et al., (2021). Persistent exertional intolerance after COVID-19: Insights From invasive cardiopulmonary exercise testing. Chest. In Press. http://doi.org/10.1016/j.chest.2021.08.010
Wagner PD (1996). Determinants of maximal oxygen transport and utilization. Annual Review of Physiology, 58(1), 21-50. http://doi.org/10.1146/annurev.ph.58.030196.000321
Wagner PD (2000). New ideas on limitations to VO2max. Exercise and Sport Sciences Reviews, 28(1), 10-14.