Background
Hypertension is frequently associated with hypercalciuria1,2, nephrolithiasis3 and low bone mineral density4. Familial Hyperkalaemic Hypertension (FHHt) causes hypercalciuria5, although complications of this are not reported.
Methods
We examined a cohort of 9 patients with genetically confirmed FHHt. Biochemical, radiological, and clinical data was obtained in patients before and after thiazide treatment. All patients gave informed consent. The study had ethics committee approval (REC 05/Q0508/6). Data were compared using paired t tests or Wilcoxon paired rank tests.
Results
5 of the 9 patients were female (median age 41.7 years). The genetic diagnosis was confirmed in all patients, 5 patients had variants in KLHL3, 3 patients had variants of WNK4, and one had a variant of WNK1 (table 1).
Pre-treatment potassium was high (median 5.6 IQR 5.2-6.2 mmol/L). Pre-treatment calcium was in the normal range (2.34 IQR 2.29-2.38 mmol/L). There was significant hypercalciuria with a raised urinary calcium/creatinine ratio (0.69 IQR 0.41-1.13). However, PTH (4 IQR 3.95-4.35 pmol/L), phosphate (1.15 IQR 1.25mmol/L) and alkaline phosphatase (57 IQR 45-84 mmol/L) were all in the normal range.
Thiazide treatment significantly reduced hypercalciuria (calcium/creatinine ratio 0.15 IQR 0.05-0.29 p=0.04) as well as the serum potassium (3.9 IQR 3.5-4.4 mmol/L p=0.0167) (table 1).
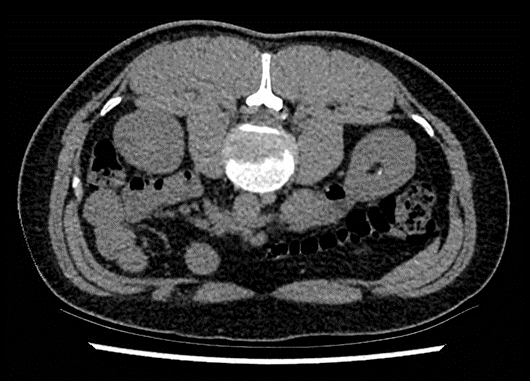
Patients also developed complications of hypercalciuria. 3 patients had kidney stones demonstrated on cross-sectional imaging (figure 1). One of these patients (male, 30 years old) had DXA criteria for osteoporosis (T score Femoral neck -1.5, lumbar spine -2.4).
Conclusion
This is the first case series to demonstrate complications of hypercalciuria (i.e. kidney stones) in patients with FHHt. We demonstrate that thiazide treatment normalises urinary calcium excretion. Thiazide treatment may have clinical utility in FHHt even if hypertension or hyperkalaemia are not problematic in order to avoid the complications of hypercalciuria.
| Demographic Data | Frequency (n of patients) | ||
| Total cohort | 9 | ||
| Female | 4 | ||
| Genetic mutation | |||
| KLHL3 | 5 | ||
| WNK4 | 3 | ||
| WNK1 | 1 | ||
| Thiazide diuretic | 3 | ||
| Nephrolithiasis | 3 | ||
| Osteoporosis | 1 | ||
| Laboratory Data | Pre-thiazide | Post-thiazide | p-value |
| K (mmol/L) median | 5.6 | 3.9 | 0.0167 |
| uCa/Cr median | 0.69 | 0.15 | 0.04 |