Introduction: Acidosis is associated with exacerbated loss of kidney function in chronic kidney disease (CKD). Currently, acid/base status is assessed by plasma measures, although organ-damaging covert acidosis, subclinical acidosis, may be present before reflected in plasma. Low urine NH4+ excretion associates with poor renal outcomes in CKD and has been proposed as a marker for subclinical acidosis. However, a low NH4+ excretion could result from either a low capacity or a low demand for acid excretion. We hypothesized that a urine acid/base-score reflecting both the demand and capacity for acid excretion would better predict CKD progression.
Methods: 24-hour urine collections were included from three clinical studies of patients with CKD stage 3 and 4: A development cohort (n=82), a variation cohort (n=59), and a validation cohort (n=73). A urine acid/base-score was derived and calculated from urinary pH and [NH4+]. Subclinical acidosis was defined as an acid/base-score below the lower limit of the 95% prediction interval of healthy controls. Main outcomes were percentage change in measured GFR after 18 months and CKD progression (defined as ≥50% decline in eGFR, initiation of long-term dialysis or kidney transplantation) during up to 10 years of follow-up. To assess percentage change in measured GFR as a function of acid/base-score and subclinical acidosis status, log-transformed measured GFR values was analyzed as outcome variable using a mixed-effects models for repeated measures. Models included visit (baseline vs. 18 months follow-up), acid/base-score or subclinical acidosis and visit-by-acid/base-score or subclinical acidosis interaction as fixed effects. The risk for CKD progression as a function of acid/base-score and subclinical acidosis status was assessed by cox proportional hazards models. All estimates were assessed with and without adjustment for important clinical risk factors for GFR decline and CKD progression (sex, age, baseline GFR, proteinuria, systolic blood pressure, and plasma bicarbonate).
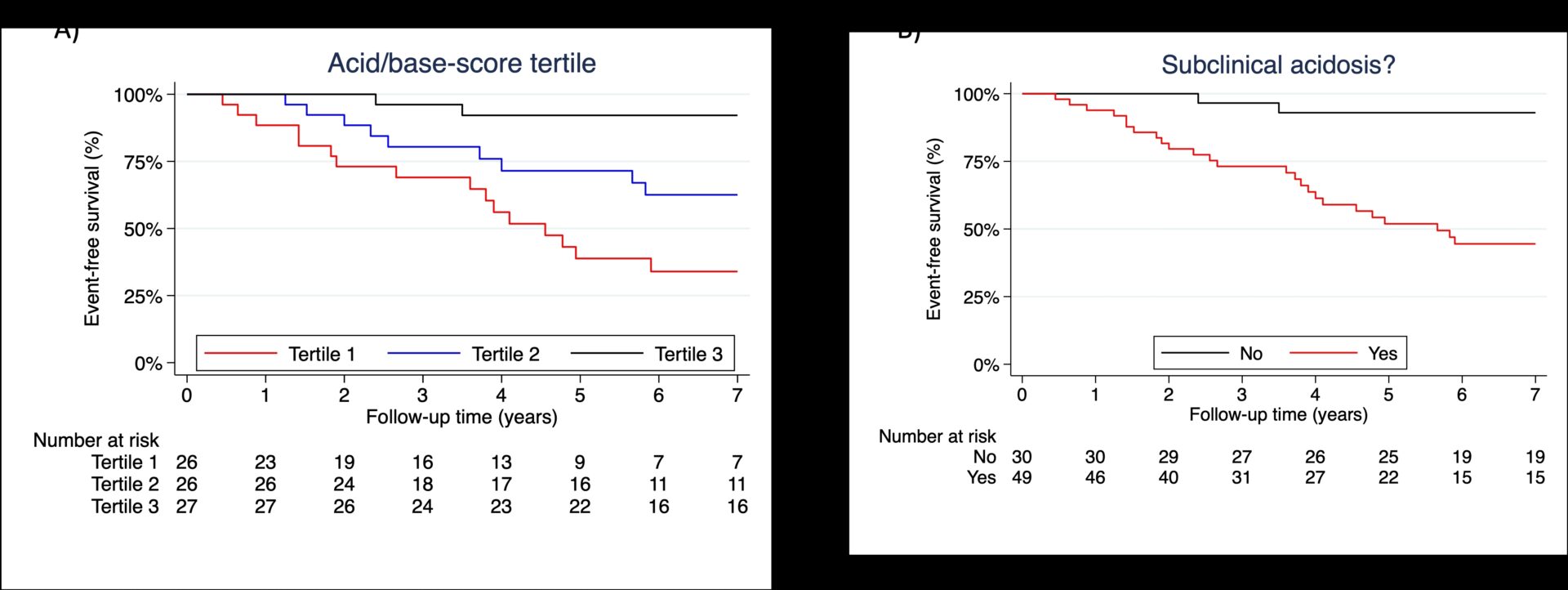
Results: Subclinical acidosis was prevalent (development cohort: n=51/82, 62%, validation cohort: n=47/73, 65%). Subclinical acidosis was associated with an 18% (95% CI: 2-32) larger percentage decrease of measured GFR after 18 months. During a median follow-up of 6 years, subclinical acidosis was associated with a markedly higher risk for CKD progression. Adjusted hazard ratios were 5.1 (95% CI 1.1-23.3) in the development cohort and 11 in the validation cohort (95% CI: 2.9-42.4). The adjusted hazard ratio in the pooled cohorts was 5.7 (95% CI: 2.3 to 14.4) for patients with subclinical acidosis. Kaplan-Meier plots for event-free survival stratified for acid/base-score tertile and subclinical acidosis are shown in figure 1. The acid/base-score had a higher predictive value for CKD progression than NH4+ excretion alone (C-score of 0.73 vs. 0.55, difference: 0.18, 95% CI: 0.05 to 0.30).
Conclusion: Subclinical acidosis, defined by a new urine acid/base-score, is associated with a higher risk of CKD progression in patients with CKD stage 3 and 4.