Introduction: Type 2 diabetes mellitus (T2DM) is a major cause of morbidity and mortality across the world. The importance of glycaemic control in T2DM is well-established and remains a key treatment target, as poor glycaemic control is associated with diabetes-related complications(1). Alongside HbA1c, best practice guidelines(2) highlight the clinical significance of short-term measures of glycaemic variability to assess glycemia in those with T2DM. Long-term adherence to dietary and behavioural strategies to manage glycaemia is often poor, so novel approaches are warranted. It is well-known that circadian rhythms play a key role in human metabolism(3). For example, glucose tolerance is typically optimal in the morning compared to later in the day. Time-restricted eating (TRE) – where energy intake is typically limited to <12 hours per day – may be a simple and effective dietary approach to the management of T2DM as it considers the importance of meal timing(4). Research thus far suggests the metabolic benefits associated with TRE are driven by the position of the eating window and studies have shown that early-TRE may promote superior metabolic benefits in healthy individuals(5). However, studies in those with T2DM are sparse.
Aims/hypothesis: To compare early versus late-TRE in adults with T2DM. We hypothesised that a daily 16-hour fast would lower mean 24-hour glucose concentration and improve other markers of glycaemic control, in individuals with T2DM. We hypothesised that these changes would be greater following early-TRE than late-TRE.
Methods: This study received a favourable ethical opinion from the University of Surrey Ethics Committee. Written informed consent was obtained prior to screening participants for eligibility for this 9-day cross-over, controlled eucaloric dietary intervention study. Eligible participants (n = 8) were fitted with continuous glucose monitors and allocated to group A or group B. All participants completed a 3-day control diet (eating window [EW] 7:00h to 19:00h), then Group A followed 3 days of early-TRE (EW 7:00h to 15:00h) while Group B commenced 3 days of late-TRE (EW 12:00h to 20:00h) before crossing over. All food (3 meals per day) consumed by participants during the study period was provided by the research team.
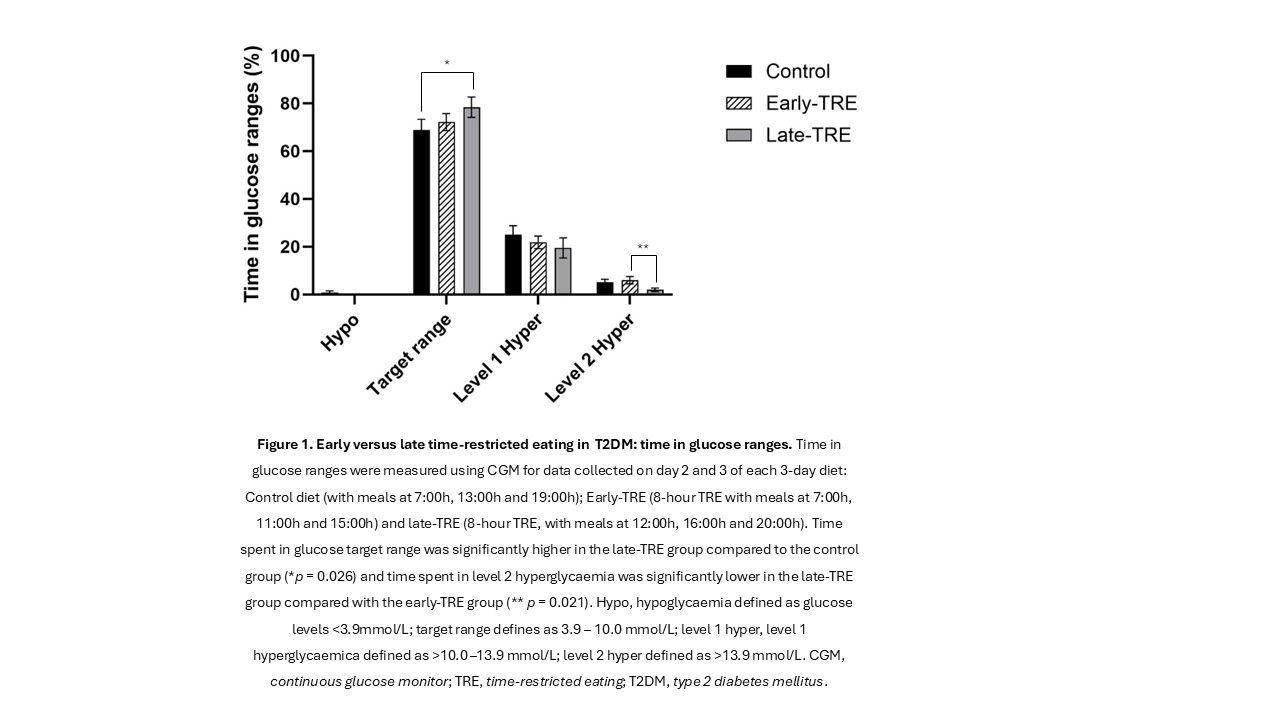
Results: Repeated measures ANOVA with post hoc tests using Bonferroni corrections were used to analyse measures of glycaemic control. Data are presented as mean ± SEM unless otherwise specified, with p<0.05 considered significant. Indices of glycaemic variability (CV and SD) were significantly lower in the late-TRE group compared to the control and early-TRE groups (CV, p<0.001 and p<0.001 respectively; SD, p = 0.007 and p = 0.003, respectively). A reduction in the 3-hour postprandial responses in the late-TRE group for meal 2 and meal 3 was observed, compared to the early-TRE group (p = 0.036 and p = 0.026, respectively). Late-TRE, but not early-TRE, increased time in glucose target range (3.9-10.0 mmol/L) – 78.4 ± 4.2 % in the late-TRE group compared to 68.9 ±4.4 % in the control group (p = 0.026) – Figure 1.
Conclusions/interpretation: Our data suggest that short-term late-TRE provides superior benefits to acute markers of glycaemic control compared with early-TRE in T2DM.