
Physiology News Magazine
Breath of the Sith: a case study on respiratory failure in a galaxy far, far away
Spoiler alert!
Features
Breath of the Sith: a case study on respiratory failure in a galaxy far, far away
Spoiler alert!
Features
Ronan Berg
Department of Clinical Physiology & Nuclear Medicine, Frederiksberg and Bispebjerg Hospitals, Copenhagen, Denmark
Ronni Plovsing
Department of Intensive Care 4131, University Hospital Rigshospitalet, Copenhagen, Denmark
https://static.physoc.org/app/uploads/2019/12/03112114/pn.103.30.figure1.jpg

While the eagerly awaited seventh instalment in the Star Wars saga has thrilled physiologists and non-physiologists alike, it may be worthwhile to take a look back at what we as respiratory physiologists have learned from the venerated space opera so far. It remains indisputable – at least between the authors of this paper – that the first six episodes’ protagonist-turned-villain-turned-saviour Anakin Skywalker/Darth Vader is the most fascinating case study on respiratory failure in the history of cinema. The enigmatic breathing sounds produced by his iconic whole-body armoured suit, as well as his mysterious underlying respiratory condition, have been source of bewilderment and fascination (and fright) to at least two aspiring respiratory physiologists that grew up in the outskirts of Denmark during the 1980s, a time when every child dreamt of becoming either a Jedi Knight or a Stormtrooper.
|
|
Department of Intensive Care 4131, University Hospital Rigshospitalet, Copenhagen, Denmark |

|
|
Department of Intensive Care 4131, University Hospital Rigshospitalet, Copenhagen, Denmark |
Health hazards of volcanic fumes
In the Star Wars saga, the highly talented Jedi knight, Anakin Skywalker, choses to abandon the monastic Jedi Order and instead join his father figure Sheev Palpatine in the more exclusive and politically involved Sith Order. As he does this, he assumes a new identity as Darth Vader, and earns the title Dark Lord of the Sith. For a number of reasons, this change of careers does not impress a former Jedi Master of his, and the two soon clash in a light sabre duel on the volcanic planet Mustafar. The confrontation results in a near-fatal outcome for Darth Vader who loses several limbs in the fight, and while he is incapacitated on the volcanic shore, he furthermore suffers inhalational injury and third degree burns. However, before he passes away, Palpatine comes to the rescue, and organises timely medical intervention.
Prior to the tragic events on Mustafar, Vader’s health and fitness level are seemingly excellent. Even though the air on a volcanic planet is mostly composed of water vapour, carbonic and sulphuric gases, and nitrogen, with insignificant levels of oxygen (Cadle 1980), Darth Vader and his former Jedi Master readily engage themselves in the intense and extremely physically challenging light sabre duel in this climate (probably the equivalent of an hour-long high-intensity exercise bout at the summit of Mount Everest), without ever taking even a short break to catch their breath. After the incident, Darth Vader is, however, unable to breathe freely at all; outside his personal meditation chamber, which also appears to function as some kind of a fancy hyperbaric oxygen facility, he continually relies on a mobile life-support system, which is integrated in a whole-body armoured suit,
in order to survive (Figure 1).
Darth Vader’s acute respiratory failure appears to be the consequence of a number of factors, including direct thermal injury to the airways, chemical damage to the lung parenchyma caused by inhalation of smoke and volcanic dust particles, carbon monoxide poisoning, as well as secondary effects to his severe third degree burns, which seems to cover ~100 % of his total body surface area.
Thermal injury caused by scalding volcanic fumes primarily affects the central parts of the lungs, because the dissipation of heat results in less damage to the peripheral areas (Eyal et al., 1975). This causes oedema in the large airways, as well as peribronchial and perivascular haemorrhages, and acutely reduces pulmonary compliance, but without any marked effects on pulmonary gas exchange within the first few hours. In addition, so-called pyroclastic density currents, volcanic gases that move laterally near the ground at hurricane velocities, may induce immediate thermal injury beyond the central parts of the lungs (Hansell et al., 2006).
Volcanic fumes furthermore contain numerous irritants that cause chemical damage to the airways (Nemery 2006). Gaseous irritants with high water solubility, such as ammonia and sulphuric dioxide, are mainly trapped in the aqueous surface of the upper respiratory tract, and give rise to immediate symptoms. They cause airway wall oedema, bronchospasm, ulcerations, and necrosis in the conductive airways. Volcanic gas irritants with a low water-solubility, such as nitrogen oxides, may pass the upper airways and eventually reach the alveolar compartment. These induce alveolar inflammation with oedema formation, and impair mucociliary function and surfactant production, but do not usually cause symptoms until after several hours. Many volcanic aerosols have an aerodynamic diameter of less than 5 µm, and are thus easily dispersed in the peripheral airways, where they may cause similar effects to gas irritants with low water solubility.
Inhalation-induced acute respiratory distress syndrome in a Sith Lord
Darth Vader’s immediate respiratory distress on the volcanic shore is probably caused by volcanic gaseous irritants with high water solubility in the volcanic fumes, which cause immediate symptoms of tracheobronchitis, and impair pulmonary gas exchange (Nemery 2006; Mlack et al., 2007). Since Darth Vader may concurrently be exposed to high levels of carbon monoxide, which both impairs the red blood cell uptake of oxygen in the lungs due to its higher affinity for haemoglobin than oxygen, and furthermore shifts the oxygen-haemoglobin saturation curve to the left, so that the release of oxygen from the red blood cells to tissue mitochondria (and perhaps also the conceivably similar midi-chlorians) in various organs is impaired; severe tissue hypoxia therefore ensues. Due to his quite severe facial burns, it is difficult to determine whether Darth Vader exhibits ‘cherry-red cheeks’ at this stage, a typical clinical finding associated with carbon monoxide poisoning, but his rather agitated emotional state is characteristic of the cerebral dysfunction often encountered in this clinical condition.
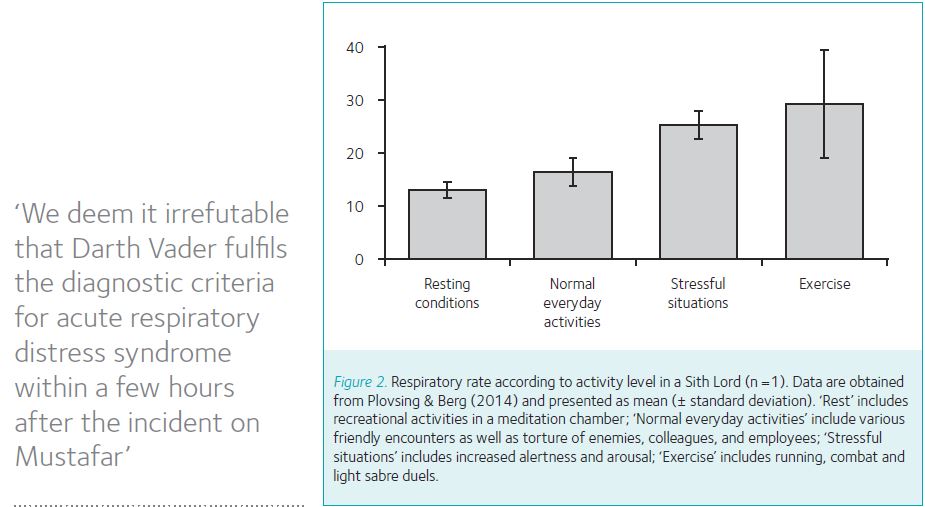
Within a few hours, that is, after Darth Vader has been evacuated by Palpatine, the effects of direct thermal injury on the central parts of the lungs, as well as the effects of the volcanic water soluble gaseous irritants and aerosols set in. These give rise to acute chemical pneumonitis with non-cardiogenic pulmonary oedema and induce a reduction in ventilatory capacity with increased pulmonary ventilation-perfusion inequality, thus severely impairing pulmonary gas exchange (Nemery 2006). At this stage, the systemic inflammatory response to the severe skin burns may furthermore disseminate from the blood stream to the alveolar compartment, and thus exaggerate the pulmonary inflammatory response. Although appropriate diagnostic imaging would be required to establish the diagnosis here on Earth, we deem it irrefutable that Darth Vader fulfils the diagnostic criteria for acute respiratory distress syndrome within a few hours after the incident on Mustafar, which is a common complication both after inhalation injury and severe skin burns (Mlack et al., 2007).
Following extensive robotic surgery, the medical droids choose to treat Darth Vader’s respiratory condition by means of the iconic whole-body armoured suit. The suit contains a mobile life-support system, and from a careful analysis of Episodes IV-VI, we have concluded that it functions as an advanced bi-level positive airway pressure (BPAP) system that supports Darth Vader’s intrinsic breathing both during in- and expiration, while preventing airway collapse, and continually supplying him with oxygen (Plovsing & Berg 2014). Accordingly, his respiratory rate varies with his activity level (Figure 2), and pressure equalisation with the surroundings can clearly be heard when his helmet is detached. Other scientists have noted that Darth Vader’s whole-body armoured suit may furthermore function as a means of preventing infections, which is notably relevant in the immediate aftermath of the events on Mustafar, due to Darth Vader’s extensive skin burns (Perrella et al., 2015).
Dark Lord of the Sith: A blue bloater in disguise?
Studies have shown that patients with acute respiratory distress syndrome, including those that involve thermal and/or inhalational lung injury, suffer from permanent reductions in ventilatory capacity as well as impaired pulmonary gas exchange after discharge from hospital (Neff et al., 2003). This also appears to be the case for Darth Vader, despite the timely intervention by Palpatine’s medical droids. Hence, as we encounter Vader in Episode IV, two decades after the events on Mustafar in Episode III, it is clear that the treatment with the whole-body armoured suit has been maintained during all the intervening years.
Since Darth Vader continually relies on the whole-body armoured suit, the acute effects of the thermal and chemical injury must have led to lung fibrosis due to extensive scar tissue formation in the pulmonary parenchyma, which permanently reduces ventilatory capacity on a restrictive basis and impairs gas exchange by increasing ventilation-perfusion inequality (Plovsing & Berg, 2014). It is less clear whether he also suffers from chronic bronchitis, which could add a obstructive component to his lung disease. In contrast to General Grievous, the Supreme Commander of the Confederacy of Independent Systems during the Clone Wars, who is a clear-cut case of chronic bronchitis with a rattling cough, Darth Vader is never once observed to cough during the Star Wars saga. On the other hand, he clearly has the appearance of a ‘blue bloater’ with bluish colour of the skin and lips, and develops severe wheezing when Luke Skywalker detaches his mask in Episode VI (Figure 3). These are characteristic features of chronic bronchitis, and the lack of coughing from the Sith Lord thus rather reflects the efficacy of the treatment with the whole-body armoured suit than it reflects absence of obstructive pulmonary disease.
Conclusion
Our extensive analysis of the first six instalments of the Star Wars saga demonstrates that Darth Vader suffers from the chronic aftermath of acute respiratory distress syndrome caused by inhalation-injury and skin burns, which is treated by a whole-body armoured suit that features an advanced BPAP system. The findings of our study stress that volcano-associated pulmonary injury is far from trivial, and furthermore that acute respiratory distress syndrome and its complications are diagnostic entities that extend way beyond the traditional intensive care setting.

References
Cadle RD (1980). A comparison of volcanic with other fluxes of atmospheric trace gas constituents. Rev Geophys 18, 746-52
Hansell AL, Horwell CJ, Oppenheimer C (2006). The health hazards of volcanoes and geothermal areas. Occup Env Med 63, 149-56
Eyal Z, Dunsky EH, Polliack A, Davidson JT (1975). The acute effect of pulmonary burns on lung mechanics and gas exchange in the rabbit.
Br J Anaesth 47, 546-52
Mlcak RP, Suman OE, Herndon DN (2007). Respiratory management of inhalation injury.
Burns 33, 2-13
Neff TA, Stocker R, Frey HR, Stein S, Russi EW (2003). Long-term assessment of lung function in survivors of severe ARDS. Chest 123, 845-853
Nemery B (2006). Chemical-induced lung injury and its long-term sequelae. In: Imaging of Occupational and Environmental Disorders of the Chest. Springer Berlin Heidelberg, pp. 67-75.
Perrella A, Russo C, Giuliani A, Esposito C, Saturnino P (2015). Infection control in a far, far away Galaxy: new and alternative learning tool from popular
culture to improve the antimicrobial stewardship.
North Am J Med Sci 7, 236-7
Plovsing RR, Berg RMG (2014). Pulmonary pathophysiology in another galaxy.
Anesthesiology 120, 230-2