Background:
Muscle wasting and weight loss are systemic manifestations of chronic obstructive pulmonary disease (COPD), particularly in those with severe airflow obstruction. Sedentarism, appetite changes, oxidative stress, inflammation, and tissue hypoxia contribute to sarcopenia in COPD [1]. Low fat-free mass index (FFMI) and BMI are associated with poor outcomes, including increased mortality [2]. Despite elevated energy requirements, malnutrition is prevalent in up to 30% of COPD patients, particularly in inpatients and advanced disease. However, little is known about the nutritional status of younger, mild-to-moderate COPD patients in outpatient settings [3].
Objective:
To assess energy and protein intake, body composition, and functional capacity in mild-to-moderate COPD patients compared with healthy non-smoking individuals (HNS).
Methods:
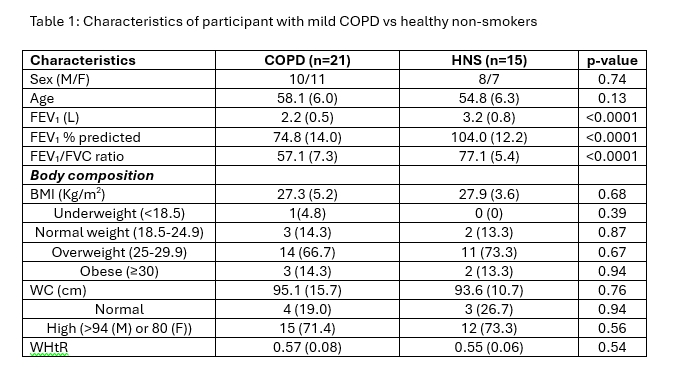
COPD participants (mean age 58.1 years) had FEV1/FVC <0.7 and FEV1 ≥50% predicted (mean 74.8%). All were current or former smokers with ≥10 pack years; 50% used inhaled corticosteroids. HNS (mean age 54.8 years) were age- and sex-matched non-smokers with normal lung function. Functional capacity was assessed using Short Physical Performance Battery (SPPB: standing balance, 4-meter gait speed (4MGS), and five-repetition sit-to-stand motion (5STS)), 6 Minute Walk Test (6MWT), Timed Up and Go (TUG) and Handgrip Strength (HGS).
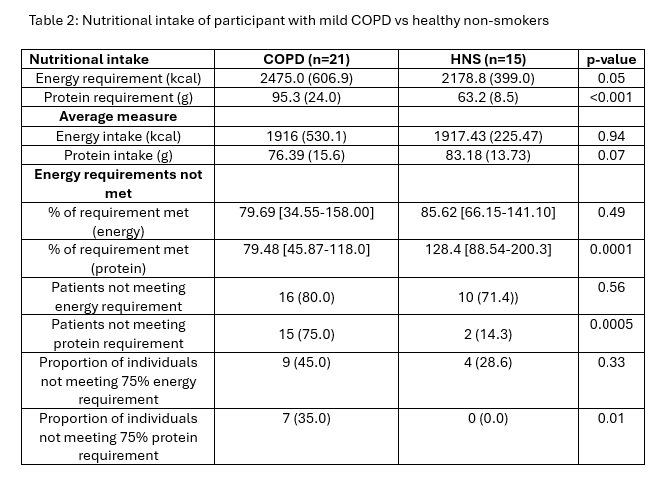
Energy and protein intakes were measured using the EPIC-Norfolk Food Frequency Questionnaire and a 7-day food diary, analysed with FETA [4] and Nutritics software [5]. Participants not meeting ≥75% of estimated requirements were classified as nutritionally inadequate. Body composition was assessed using bioelectrical impedance analysis; low FFMI was defined as <15 kg/m² (females) and <17 kg/m² (males). Proportion of participants not meeting protein and energy requirements were calculated using PENG guidelines [6]. Comparisons between groups were assessed using independent t-tests, Mann-Whitney U tests, or Chi-squared tests, as appropriate. See Tables 1 and 2
Results:
Body composition did not differ significantly between COPD and HNS (%FFM: 66.8 vs. 69.3; FFMI: 18.9 vs. 19.1 kg/m²). A higher, though non-significant, proportion of COPD patients had low FFMI (9.5% vs. 0%, p=0.22). Most participants were overweight (BMI >25 kg/m²), and ~75% showed high central adiposity.
Mean daily energy intake was similar between groups (COPD 1857 kcal vs. HNS 1917 kcal, p=0.64). Protein intake was lower in COPD (75.7 g vs. 83.2 g, p=0.14). Significantly more COPD patients did not meet protein requirements (75% vs. 14%, p<0.01), and 35% consumed <75% of estimated needs. In COPD, both energy and protein intake correlated moderately with SPPB performance (r=0.57, p=0.02; r=0.50, p=0.049), but not with other functional measures.
Conclusions:
Younger, mild-to-moderate COPD patients often present as overweight with excess central fat yet demonstrate inadequate protein intake. Despite preserved body composition, low dietary protein may predispose this group to future sarcopenia. Since overweight status can mask muscle loss, nutritional risk may be overlooked in clinical care. Early multidisciplinary intervention, including dietary assessment and targeted nutritional support, may help prevent sarcopenia progression in this population.